
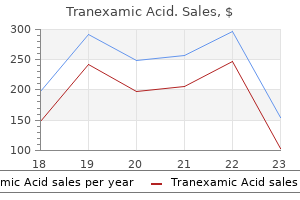
Tranexamic Acid dosages: 500 mg
Tranexamic Acid packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Order tranexamic 500mg with visa
These filaments are connected to the cytoplasmic plaques at the areas of cell-to-cell junctions corresponding to desmosomes and hemidesmosomes. In basic, they play a serious practical function in preserving cell structural integrity and mechanical stability. They are additionally essential elements of cell-to-cell and cell-to-stroma interactions. Moreover, epithelia in several organs have different compositions of their keratin, and their expression is retained to some extent in neoplasms derived from these organs. A, Classification of intermediate filaments based on sequence homology and cell-type specificity of their expression patterns. B, Schematic representation of the common tripartite domain construction for all intermediate filaments. A central rod-domain is comprised of heptad repeat-containing -helical coils 1A, 1B and 2A, 2B. The central rod area is flanked by head and tail domains of variable length and structure at their N- and C-termini. C, Assembled 10-nm wide intermediate filament buildings reconstituted from recombinant protein visualized by adverse staining and transmission electron microscopy. Examples of positivity for keratin have been described for nearly each nonepithelial tumor, together with many bone tumors. Still, for sensible purposes, a robust, uniform positivity of tumor cells for keratin typically is seen in epithelial tumors. Vimentin is a 57-kDa filamentous protein universally expressed in mesenchymal cells and in some epithelial cells and their neoplasms. For these two causes, the specific diagnostic applicability of vimentin within the differential diagnosis of tumors is minimal. It is most frequently used to verify the antigenicity of cells in question when other markers are adverse. Desmin can also be expressed in some fetal cells, similar to embryonal mesothelium, stromal cells of fetal kidney, and chorionic villi. In mammalian skeletal muscle, together with in people, desmin is amongst the earliest proteins expressed in muscle lineage differentiation and can be detected in somites and early myoblasts. Typically, all three polypeptides are expressed, however some neuronal cells could lack all or a few of the neurofilament proteins. In common pathology, neurofilaments are used as markers of neural differentiation. Poorly differentiated tumor cells might categorical undetectable levels of neurofilament protein. Moreover, fixation and paraffin embedding significantly cut back the stainability of cells for this marker. Epithelial Markers Keratins are the markers most regularly used in the identification of epithelial phenotypes (see the part on intermediate filaments). It is an indispensable component of cell integrity, form, and motion in all eukaryotic cells. The F-actin is a singular polar structure that incorporates a fast-expanding polymerizing plus-end and a minus-end by which depolymerization (referred to as treadmilling) happens. Actin binds quite a few partners that participate in varied biologic capabilities concerned in cell motility and signal transductions. Actins are divided into three main subgroups of comparable molecular weight, 42-kDa:, and. The three forms of actin are organ or tissue specific and are designated as -skeletal, -cardiac, and -smooth muscle. On the opposite hand, the expressions of actins (skeletal, cardiac, and smooth muscle) in addition to �smooth muscle actin are tissue specific. Histochem Cell Biology 129:705-733, 2008 based mostly on new consensus nomenclature from Schweizer J et al. This expression sample makes desmin one of the useful markers of muscle differentiation. In pathology, desmin is used as a marker for the diagnosis of tumors that exhibit muscle, predominantly skeletal, differentiation.
Discount tranexamic online visa
Lymphangiomatosis predominantly happens in children and barely turns into manifest after age 20 years. Diagnosis at start is unusual; a latent period is required for lesions to obtain adequate measurement to turn out to be symptomatic. The lesion also can occasionally present as a pathologic fracture, particularly in the lengthy bones. The lesions appear to be composed of multiple coalescent lytic areas separated by skinny sclerotic zones. The use of lymphangiography helps establish the character of the lesion earlier than biopsy. Some cases of lymphangiomatosis of bone can pursue an aggressive medical course with progressive bone loss (massive osteolysis) and will have radiographic features of disseminated generalized illness (cystic angiomatosis). Regional angiomatosis entails one or several bones of the identical anatomic region. Disseminated generalized angiomatosis, also referred to as cystic angiomatosis, is a generalized multifocal disorder that predominantly entails the trunk bones. Aggressive angiomatosis, or large osteolysis, is a peculiar type of angiomatosis that progressively destroys (lyses) the affected bone or bones. Cystic Angiomatosis the time period cystic angiomatosis is utilized to extremely rare conditions of disseminated multifocal hemangiomas in the skeleton. The sites of extraskeletal involvement embrace delicate tissue, lung, liver, and particularly spleen. The condition could be asymptomatic and is commonly detected by the way in radiographs obtained for different causes. Radiolucent lesions with a soap-bubble or honeycomb look are present within the skull, spine, ribs, and pelvis. In rare cases, the disorder is manifested on radiographs as disseminated osteoblastic lesions that mimic osteoblastic metastases. A and B, Lymphangiomatosis of the rib showing cortical bone eroded by medullary lymphangiomatous process composed of dilated, endothelial-lined channels. C and D, Dilated lymphatic channels of varying sizes forming a spongy structure throughout the medullary bone. A, Radiograph of fibula reveals space of cortical enlargement with coarse trabeculation. B, Gross photograph of bivalved resection phase of fibular shaft shows localized area of honeycomb appearance situated eccentrically in cortex. C and D, Low and intermediate power photomicrographs of lymphangioma of bone show dilated, endothelial-lined channels with delicate walls. A, Chest radiograph of a 7-year-old boy with lymphangiomatosis of a number of right ribs and right-sided chylous effusion. B, Coarse trabeculation of a quantity of ribs on right aspect was produced by lymphangiomatosis. C, Computed tomogram of chest shows chylous effusion and rarefaction of posterior portion of rib. On radiographs, lytic lesions could additionally be seen to comprise some residual lamellar bone and foci of reactive woven bone. Blastic lesions contain distinguished, thickened bone trabeculae of mature lamellar bone with areas of woven bone rimmed by osteoblasts. Evaluation of serial radiographs on this disorder has proven that growing osteosclerosis can be an age-related phenomenon in angiomatous foci which may be originally lytic. It could additionally be that the lesions spontaneously heal or regress and that this course of is accompanied by sclerosis. Rare circumstances of angiosarcoma arising from skeletal angiomatosis have been described. Usually, it entails the shoulder and hip areas and starts within the trunk bones, and it could individually contain a number of bones in the same region. In the appendicular skeleton, the proximal parts of the extremity bones-the proximal humerus and femur-are usually concerned. They are indistinguishable from odd, nonaggressive angiomatoses and characterize a fancy Text continued on p. B, Multiple lucent areas with coarse trabeculation involving patella, proximal tibial metaphysis and epiphysis, and proximal fibular shaft in teenaged patient.
Generic tranexamic 500 mg mastercard
A, Radiograph of sclerotic nidus in proximal phalanx of long finger (arrows) of a 26-year-old lady who noted ache and swelling for two years earlier than prognosis was established. She had been followed and treated for suspected osteomyelitis all through this period. B, Clinical photograph of case A exhibiting delicate tissue edema and deformity of lengthy finger. C, Radiograph exhibiting lucent nidus with sclerosis in the adjoining bone in proximal phalanx of fifth finger. D, Radiograph of a 22-year-old man with pain, swelling of soppy tissue, and expanded radiolucent nidus in proximal phalanx of index finger (arrows). Diagnosis of chronic osteomyelitis resulted in extended therapy with antibiotics. Cultures have been at all times unfavorable, and even after synovial biopsy, persistent inflammation was identified. Finally, after 5 years radiologic diagnosis of osteoid osteoma was instructed, and curettage resulted in everlasting relief of signs. A, Radiograph of elbow joint with diffuse, poorly demarcated space of sclerosis of proximal ulnar metaphysis (arrows). C, Radiograph of elbow exhibiting ill outlined sclerosis and prominent periosteal reaction involving the distal finish of humerus. D, Magnetic resonance imaging shows inhomogeneous subarticular nidus of intermediate signal depth (arrows). Note prominent periosteal reaction of the distal humerus and fluid accumulation in the elbow joint. A, Lymphoproliferative synovitis with lymphocytic infiltrate of synovium and a number of lymphoid follicles with germinal centers. Note scattered predominantly perivascular inflammatory infiltrate (A, �50; B, �100) (A and B, hematoxylin-eosin) four Benign Osteoblastic Tumors 167 Personal Comments Problems with the identification of nidus tissue and the simulation of reactive, posttraumatic, and inflammatory situations have predominated in diagnostic case material submitted for session. The humoral effects of osteoid osteoma on surrounding bone and soft tissue have often masked the presence of a nidus and have led to lengthy delays in prognosis and therapy. As a consequence, the affected person could endure inappropriate remedy for a lot of months and even years under the mistaken diagnostic impression of an infection or inflammatory situation. Frequent use of computerized imaging methods in diagnostic workup in bone lesion in modern apply has dramatically lowered the incidence of such lesions. The male/female ratio is the same as that for osteoid osteoma, roughly 2: 1. Benign osteoblastoma also occurs frequently within the extremities, the place its overall distribution is similar to that of osteoid osteoma. Consequently the proximal femur in the area of the femoral neck is its most frequent website within the appendicular skeleton. Rare situations of osteoblastomas associated with severe systemic symptoms of fever, weight reduction, cachexia, clubbing of fingers and toes, and diffuse periostitis ("poisonous osteoblastoma") have been observed. Benign osteoblastoma produces a round or oval, well-demarcated metaphyseal lytic defect surrounded by a zone of reactive sclerosis. It is believed that the predilection of benign osteoblastoma for cancellous bone could a minimum of in part account for the absence of distinct sclerosis. Extensive reactive changes within the surrounding tissue and apparent delicate tissue lots on magnetic resonance imaging may overestimate the extent of the lesion, so computed tomography should continue to be the imaging modality of selection for the demonstration and local staging of suspected vertebral osteoblastomas. Their pathogenetic relationship to the foundation of the tooth is most likely incidental. In truth, the microscopic features of the nidus in osteoid osteoma are comparable and very often equivalent to those of osteoblastoma. Benign osteoblastoma differs from osteoid osteoma in that it has the next growth potential as a end result of it exceeds 2 cm in diameter. Moreover, it regularly lacks distinct nocturnal pain that could be relieved by aspirin. Still, there are cases with composite options that fall between osteoid osteoma and osteoblastoma. This downside has been resolved by arbitrarily designating all lesions as osteoblastomas when the nidus is more than 1. The lesion designated as cementoblastoma in the oral pathology literature is an osteoblastoma positioned in jaw bones within the vicinity of the roots of teeth.
Generic tranexamic 500 mg without prescription
A-D, Hypercellular hyaline cartilage mass on the floor of osteochondroma consistent with a secondary chondrosarcoma. A-D, Hypercellular cartilage with atypical cartilage cells consistent with a secondary chondrosarcoma related to osteochondroma. Bonnevialle P, Mansat M, Durroux R, et al: Chondromas of the hand: a report of 35 circumstances. Gunawan B, Weber M, Bergmann F, et al: Clonal chromosome abnormalities in enchondromas and chondrosarcomas. Matysiakiewicz J, Tomasik P, Miszczyk L, et al: Manifestations, analysis and surgical therapy of enchondroma-own expertise. Morii T, Mochizuki K, Tajima T, et al: Treatment end result of enchondroma by easy curettage without augmentation. Schajowicz F: Tumors and tumorlike lesions of bone, ed 2, Berlin, 1994, Springer-Verlag. Hagiwara Y, Hatori M, Abe A, et al: Periosteal chondroma of the fifth toe-a case report. Inoue S, Fujino S, Kontani K, et al: Periosteal chondroma of the rib: report of two cases. Karabakhtsian R, Heller D, Hameed M, et al: Periosteal chondroma of the rib-report of a case and literature evaluation. Lisanti M, Buongiorno L, Bonnicoli E, et al: Periosteal chondroma of the proximal radius: a case report. Luevitoonvechkij S, Arphornchayanon O, Leerapun T, et al: Periosteal chondroma of the proximal humerus: a case report and evaluate of the literature. Mandahl N, Mertens F, Willen H, et al: Rearrangement of band q13 on each chromosomes 12 in a periosteal chondroma. Yildirim C, Ynay K, Rodop O, et al: Periosteal chondroma that introduced as a subcutaneous mass within the ring finger. Kozlowski K, Brostrom K, Kennedy J, et al: Dysspondyloenchondromatosis in the newborn. Maffucci A: Di un caso di enchondroma et angioma multiplo: contribuzione alla genesi embrionale dei tumori. Spranger J, Kemperdieck H, Bakowski H, et al: Two peculiar types of enchondromatosis. Zack P, Beighton P: Spondyloenchondromatosis: syndromic id and evolution of the phenotype. Wang P, Dong Q, Zhang C, et al: Mutations in isocitrate dehydrogenase 1 and a couple of occur regularly in intrahepatic cholangiocarcinomas and share hypermethylation targets with gliobastomas. Evidence of mitogenic neurotransmitters present in enchondromas and gentle tissue hemangiomas. Aigner T, Loos S, Inwards C, et al: Chondroblastoma is an osteoid-forming, but not cartilage-forming neoplasm. Akai M, Tateishi A, Machinami R, et al: Chondroblastoma of the sacrum: a case report. Azorin D, Gonzalez-Mediero I, Colmenero I, et al: Diaphyseal chondroblastoma in an extended bone: first report. Edel G, Ueda Y, Nakanishi J, et al: Chondroblastoma of bone: a clinical, radiological, mild and immunohistochemical examine. Fadda M, Manunta A, Rinonapoli G, et al: Ultrastructural look of chondroblastoma. Mii Y, Miyauchi Y, Morishita T, et al: Ultrastructural cytochemical demonstration of proteoglycans and calcium within the extracellular matrix of chondroblastomas. Ozkoc G, Gonlusen G, Ozalay M, et al: Giant chondroblastoma of the scapula with pulmonary metastases. Romeo S, Szyhai K, Nishimori I, et al: A balanced t(5;17) (p15;q22-23) in chondroblastoma: frequency of the rearrangement and evaluation of the candidate genes. Sailhan F, Chotel F, Parot R, et al: Chondroblastoma of bone in a pediatric population. Schajowicz F, Gallardo H: Epiphyseal chondroblastoma of bone: a clinicopathological examine of 69 circumstances.
Tranexamic 500 mg online
These issues usually occur in very younger patients whose symptoms begin earlier than age 5 years. Long-standing hyperemia induced by prostaglandins is probably a think about accelerated growth of bone in osteoid osteoma. The ensuing bone deformity and discrepancy in limb size may disappear after excision of the nidus. In some patients, however, the deformity and length discrepancy by no means utterly resolve. However, this method is mostly discouraged because of the danger of incomplete elimination of the nidus and recurrence of symptoms. Recurrence might often occur a few years after elimination of the primary lesion. According to Mayo Clinic information, this happens in nearly 20% of patients with osteoid osteomas that have a radiologically documented nidus. The nidus tissue could be found in a relatively excessive proportion of sufferers who bear further surgical procedure. Although en bloc excision is the preferred therapy, in some cases a lesion could additionally be inaccessible to the surgeon. In such cases, its complete removing could cause extra disability than that related to the original disease. Some of those sufferers could be managed with extended treatment with nonsteroidal anti-inflammatory medication. As reported by Kneisl and Simon,65 prolonged anti-inflammatory remedy (30-40 months) can induce everlasting aid of signs, and regression of the nidus could additionally be seen on radiographs. Ablation of the nidus with a percutaneously positioned radiofrequency electrode that produces thermocoagulation has turn into extensively accepted. Reported success rates for remedy by thermocoagulation with radiofrequency electrodes have ranged between 80% and 90% (no want for additional procedures or drugs for two years). A, Radiograph of hip of an 8-year-old girl exhibits nidus with reasonable bone sclerosis surrounding lesion. B, Computed tomogram at this level exhibits nidus extra clearly with cortical thickening and medullary sclerosis. C, Bone scan shows large zone of elevated uptake corresponding to nidus and perilesional sclerosis. D, Radiograph of a 17-yearold athletic boy with proximal leg ache and localized cortical thickening that on the beginning was thought to symbolize a stress fracture. E, Computed tomogram of tibia shown in D reveals punctate lucency diagnostic for intracortical osteoid osteoma. A, Osteoid osteoma of the proximal humerus with prominent diffuse sclerosis and periosteal reaction deforming bone contour. B, Anteroposterior radiograph exhibiting diffuse sclerosis and size discrepancy of the left femur. Note sclerosing lesion of left tibial diaphysis and pronounced length discrepancy. F, Clinical photograph of the identical patient 1 12 months later, exhibiting discrepancy in limb length and protracted bowing deformity of involved tibia. Osteoid osteomas of small peripheral bones are almost at all times associated with a distinct swelling of soppy tissue and synovitis of the adjoining joints. Therefore on this location, long delays in arriving on the appropriate prognosis could occur because the tumor may frequently mimic an inflammatory process. Osteoid Osteoma of Vertebral Column Approximately 10% to 15% of osteoid osteomas occur within the vertebral column. Spinal lesions are troublesome to detect on plain radiographs and are identified to be responsible for unexplained backache and painful scoliosis. It is beneficial that an underlying osteoid osteoma be dominated out in nearly all circumstances of unexplained again pain and painful scoliosis that occur in kids and young adults. At best, the radiographs may show an space of sclerosis, a thickened and distorted sclerotic transverse course of, or a deformed sclerotic pedicle with indistinct borders. Magnetic resonance imaging also may facilitate the identification of an inconspicuous nidus. High sign in T2weighted images of nidus tissue correlates properly with its elevated vascularity.
Discount tranexamic 500mg free shipping
C and D, Intermediate and high energy photomicrographs exhibiting myxoid and hyaline chondroid matrix formation. Note pronounced cellular variability and nuclear hyperchromasia (A and B, �25; C, �100; D, �200) (A-D, hematoxylin-eosin). A and B, Low and medium power photomicrographs of chondroid metaplastic nodules within the synovium. C and D, Medium and excessive power photomicrographs displaying loosely arranged cells with chondroblastic options within myxoid areas adjacent to discrete cartilage nodules. It is our impression that immaturity of cartilage cells is answerable for prominent atypia in a majority of circumstances. Enchondral ossification of cartilage nodules is a frequent feature of well-developed synovial chondromatosis. Occasionally the nodules consist of well-formed rings of lamellar bone with a central, fatty bone marrow�like space. Lesions with welldeveloped enchondral ossification are additionally referred to as osteochondromatosis. Lesions that current as a single cartilaginous nodule within the joint capsule are generally referred to as synovial chondromas. It is still controversial whether or not a single discrete nodule within synovium or periarticular soft tissue is a clonal neoplastic proliferation of cartilage cells. Differential Diagnosis an important consideration in differential analysis is chondrosarcoma. The cytologic atypia of cartilage cells is usually worrisome and raises the suspicion of chondrosarcoma. The method used to evaluate synovial chondromatosis is similar as that used to consider cartilage lesions of bone. Thus as with cartilage lesions, all scientific and radiographic findings must be considered. First, rare but well-known secondary involvement of the joint by a chondrosarcoma of the adjoining bone, such because the femur or tibia, must be clinically and radiographically ruled out. This dilemma arises most incessantly in evaluating hip lesions, during which the joint capsule may be secondarily involved by a chondrosarcoma of the adjoining pelvic and femoral bones. When the medical, radiographic, and gross findings are consistent with the process confined to the joint capsule and area, the atypia of cartilage cells can be discounted as a feature of malignant transformation, and the lesion can be categorised as synovial chondromatosis. However, these circumstances must be differentiated from extremely uncommon main synovial chondrosarcoma or chondrosarcoma growing in synovial chondromatosis (see later section). In rare instances synovial chondromatosis might develop in a bursa overlying an osteochondroma. Such cases could, radiographically, mimic a secondary chondrosarcoma arising in the cartilaginous cap of the osteochondroma. Removal of the unfastened bodies and of the concerned synovium is enough to control the disease in the majority of instances. Multiple and sometimes short-interval recurrences elevate suspicion of synovial chondrosarcoma. In a sequence of 10 reported instances, solely 2 had been primary lesions, and the remaining eight developed in a setting of synovial chondromatosis. Knee involvement is the most frequent, followed by involvement of the ankle and hip. Synovial chondrosarcoma might develop in other major joints of the higher extremities and in the smaller joints of the acral skeleton. Our expertise is restricted to three cases that involved the knee, elbow, and foot. Radiographically, chondrosarcomas of the synovium ought to be suspected if a consolidated calcified mass is present in the joint area. In most circumstances, the presence of a calcified consolidated mass is related to bone erosion. Features such as loss of clustered development sample of cartilage cells, distinguished and uniform myxoid appearance, necrosis, and presence of spindling at the periphery of nodules should elevate the suspicion of malignancy. It is frequent for the final diagnosis of synovial chondrosarcoma to be made after several native recurrences of lesions initially thought of to be synovial chondromatosis.
Tranexamic 500 mg without prescription
Decreased cytoplasmic granules and spindle cell morphology are options of neoplastic mast cells. The nodules could additionally be composed predominantly of mast cells or may be accompanied by a big number of inflammatory cells, including lymphocytes, eosinophils, and histiocytes. A, Low energy photomicrograph showing mastocytosis with patchy infiltrates hugging trabeculae (�100). B, Higher energy photomicrograph of A showing some mast cells with spindle cell morphology and related fibrosis (�200). C, Mast cell lesion with central mixture of mast cells surrounded by lymphocytes and eosinophils (�200). D, Higher power magnification of C displaying mast cells with fried egg appearance with ample clear cytoplasm (�400). A and B, Low-power photomicrographs of skin in urticaria pigmentosa present dermal infiltration of mast cells containing metachromatic granules positive for Geimsa stain. C and D, Intramedullary infiltrates within bone of mast cells admixed with inflammatory cells and fibroblasts. Chen W, Wang J, Wang E, et al: Detection of clonal lymphoid receptor gene rearrangements in Langerhans cell histiocytosis. Kawamoto H, Wada H, Katsura Y: A revised scheme for developmental pathways of hematopoietic cells: the myeloid-based mannequin. Avet-Loiseau H, Garand R, Lode L, et al: Intergroupe Francophone du Myelome: translocation t(11;14)(q13;q32) is the hallmark of IgM, IgE, and nonsecretory a number of myeloma variants. Bartl R, Frisch B, Fateh-Moghadam A, et al: Histologic classification and staging of a number of myeloma: a retrospective and prospective examine of 674 cases. Fonseca R, Barlogie B, Bataille R, et al: Genetics and cytogenetics of a quantity of myeloma: a workshop report. Heerema-McKenney A, Waldron J, Hughes S, et al: Clinical, immunophenotypic, and genetic characterization of small lymphocyte-like plasma cell myeloma. Hideshima T, Mitsiades C, Tonon G, et al: Understanding a number of myeloma pathogenesis within the bone marrow to determine new therapeutic targets. Wiltshaw E: the pure history of extramedullary plasmacytoma and its relation to solitary myeloma of bone and myelomatosis. Shimoyama M: Diagnostic criteria and classification of clinical subtypes of adult T-cell leukaemia-lymphoma. Tsukasaki K, Hermine O, Bazarbachi A, et al: Definition, prognostic factors, remedy, and response standards of adult T-cell sixty six. Alencar A, Pitcher D, Byrne G, et al: Primary bone lymphoma- the University of Miami experience. Bazarbachi A, Suarez F, Fields P, et al: How I treat grownup T-cell leukemia/lymphoma. Xu Y, McKenna R, Doolitle J, et al: the t(14;18) in diffuse massive b-cell lymphoma: correlation with germinal center-associated markers and scientific features. Arnaud L, Gorochov G, Charlotte F, et al: Systemic perturbation of cytokine and chemokine networks in Erdheim-Chester disease: a single-center series of 37 patients. Cavalli G, Guglielmi B, Berti A, et al: the multifaceted clinical displays and manifestations of Erdheim-Chester illness: comprehensive evaluate of the literature and of 10 instances. Moulis G, Sailler L, Bonneville F, et al: Imaging in ErdheimChester illness: classic options and new insights. Destombes P: Adenitis with lipid excess in children or younger adults, seen within the Antilles and in Mali (4 cases). Gadner H, Grois N, Potschger U: Improved outcome in multisystem Langerhans cell histiocytosis is associated with remedy intensification. Gupta P, Babyn P: Sinus histiocytosis with huge lymphadenopathy (Rosai-Dorfman disease): a clinicoradiological profile of three circumstances together with two with skeletal illness. Hamels J, Fiasse L, Thiery J: Atypical lymphohistiocytic bone tumour (osseous variant of Rosai-Dorfman illness In Metabolic, degenerative and inflammatory illnesses of the bone and joints, Philadelphia, 1972, Lea & Febiger. Merad M, Ginhoux F, Collin M: Origin, homeostasis and function of Langerhans cells and other langerin-expressing dendritic cells. Minkov M: Multisystem Langerhans cell histiocytosis in youngsters: current treatment and future directions.
Cheap tranexamic american express
Foltz J, Jackson D: Osteogenic sarcoma of the mandible: a 24-year follow-up study. French Bone Tumor Study Group: Age and dose of chemotherapy as major prognostic components in a trial of adjuvant therapy of osteosarcoma combining two alternating drug combos and early prophylactic lung irradiation. Katenkamp D, Stiller D, Waldmann G: Ultrastructural cytology of human osteosarcoma cells. Kubista B, Klinglmueller F, Bilban M, et al: Microarray analysis identifies distinct gene expression profiles related to histological subtype in human osteosarcoma. Laflamme C, Curt S, Rouabhia M: Epidermal development issue and bone morphogenetic proteins upregulate osteoblast proliferation and osteoblastic markers and inhibit bone nodule formation. Lindqvist C, Teppo L, Sane J, et al: Osteosarcoma of the mandible: evaluation of nine instances. Machado I, Alberghini M, Giner F, et al: Histopathological characterization of small cell osteosarcoma with immunohistochemistry and molecular genetic support. Meister P, Konrad E, Lob G, et al: Osteosarcoma: histological analysis and grading. Nagata S, Nishimura H, Uchida M, et al: Giant cell-rich osteosarcoma of the distal femur: radiographic and magnetic resonance imaging findings. Negrin A, Bernardini M, Diana A, et al: Giant cell osteosarcoma within the calvarium of a cat. Okada K, Hasegawa T, Yokoyama R: Rosette-forming epithelioid osteosarcoma: a histologic subtype with extremely aggressive scientific conduct. Okada K, Hasegawa T, Yokoyama R, et al: Osteoarcoma with cytokeratin expression: a clinicopathological research of six cases with an emphasis on differential prognosis from metastatic most cancers. Sela J: Bone reworking in pathologic conditions: a scanning electron microscopy research. Sela J, Boyde A: Further observations on the relationship between the matrix and the calcifying fronts in osteosarcoma. Toguchida J, Yamaguchi T, Ritchie B, et al: Mutation spectrum of the p53 gene in bone and soft tissue sarcomas. Roessner A, Immenkamp M, Hiddemann W, et al: Case report 331: small cell osteosarcoma of the tibia with diffuse metastatic disease. Ryan J, Baker L, Benjamin R, et al: Long-term follow-up in the treatment of osteogenic sarcoma. Sadikovic B, Yoshimoto M, Chilton-MacNeill S, et al: Identification of interactive networks of gene expression related to osteosarcoma oncogenesis by built-in molecular profiling. Sampo M, Koivikko M, Taskinen M, et al: Incidence, epidemiology and treatment outcomes of osteosarcoma in Finland-a nationwide population-based research. Uhl M, Saueressig U, van Buiren M, et al: Osteosarcoma: preliminary results of in vivo assessment of tumor necrosis after chemotherapy with diffusion- and perfusion-weighted magnetic resonance imaging. Yamaguchi T, Toguchida J, Yamamuro T, et al: Allelotype analysis in osteosarcomas: frequent allele loss on 3q, 13q, 17p, and 18q. Yalcin B, Gedikoglu G, Kutluk T, et al: C-erbB-2 expression and prognostic significance in osteosarcoma. Yoshida H, Yumoto T, Adachi H, et al: Osteosarcoma with distinguished epithelioid features. Zou C, Shen J, Tang Q, et al: Cancer-testis antigens expressed in osteosarcoma identified by gene microarray correlate with a poor affected person prognosis. Bacci G, Ferrari S, Ruggieri P, et al: Telangiectatic osteosarcoma of the extremity: neoadjuvant chemotherapy in 24 circumstances. Bertoni F, Bacchini P, Pignatti G, et al: Telangiectatic osteosarcoma: survival in comparison with that of "conventional" osteosarcoma. Saito T, Oda Y, Kawaguchi K, et al: Five-year evolution of a telangiectatic osteosarcoma initially managed as an aneurysmal bone cyst. Sirikulchayanonta V, Jaovisidha S: Soft tissue telangiectatic osteosarcoma in a younger affected person: imaging and immunostains. Vanel D, Tcheng S, Contesso G, et al: the radiological appearances of telangiectatic osteosarcoma: a study of 14 cases.
Real Experiences: Customer Reviews on Tranexamic Acid
Mannig, 65 years: B, Focus on thicken bone trabeculae with scallop borders forming interconnecting community, signifying bone reworking incessantly seen in giant notochord rest.
Bengerd, 55 years: C, Radiograph displaying lucent nidus with sclerosis within the adjacent bone in proximal phalanx of fifth finger.
Carlos, 39 years: C, Biopsy material shows high-grade malignant fibrous histiocytoma (C, �100) (C, hematoxylin-eosin.
Jerek, 56 years: Heerema-McKenney A, Waldron J, Hughes S, et al: Clinical, immunophenotypic, and genetic characterization of small lymphocyte-like plasma cell myeloma.
Rasarus, 45 years: Mrad K, Sassi S, Smida M, et al: Osteosarcoma with rhabdomyosarcomatous element or so-called malignant mesenchymoma of bone.
Bufford, 30 years: Steelman C, Katzenstein H, Parham D, et al: Unusual presentation of congenital childish fibrosarcoma in seven infants with molecular-genetic evaluation.
Kafa, 51 years: D, Compensated polarization microscopy demonstrates optimistic birefringence of rhomboid calcium pyrophosphate dihydrate crystals.
Nefarius, 62 years: Juxtaarticular Osteoid Osteoma Osteoid osteomas situated throughout the articular capsule are rare and tough to detect.
10 of 10 - Review by N. Domenik
Votes: 62 votes
Total customer reviews: 62
References
- Marberger H: Hunterian lecture. Presented at: Royal College of Surgeons; 1975; London, England. Marei M, Fares A, Musa N, et al: Timing and outcome concerns regarding feminizing genitoplasty from the perspective of Egyptian families of girls with virilized external genitalia, Horm Res Paediatr 2015.
- Ashworth JL, Biswas S, Wraith E, Lloyd IC. Mucopolysaccharidoses and the eye. Surv Ophthalmol 2006;51:1-17.
- Gold NB, Westgate MN, Holmes LB. Anatomic and etiological classification of congenital limb deficiencies. Am J Med Genet A 2011;155A(6): 1225-35.
- Descotes JL, Rambeaud JJ, Deschaseaux P, et al: Placebo-controlled evaluation of the efficacy and tolerability of Permixon? in benign prostatic hyperplasia after exclusion of placebo responders, Clin Drug Investig 9(5):291n297, 1995.
- McNeill A, Birchall D, Straub V, et al. Lower limb radiology of distal myopathy due to the S60 F myotilin mutation. Eur Neurol. 2009;62(3):161-166.
- Jeejeebhoy KN: Clinical nutrition: 6.
- Andolfatto G, Abu-Laban RB, Zed PJ, et al: Ketamine-propofol combination (Ketofol) versus propofol alone for emergency department procedural sedation and analgesia: a randomized double-blind trial. Ann Emerg Med 59:504-512.