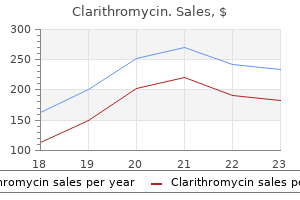
Clarithromycin dosages: 500 mg, 250 mg
Clarithromycin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Order clarithromycin 500 mg with amex
Cystoscopy can provide helpful info instantly earlier than open surgical procedure, similar to evaluation of orifice position, duplication anomalies, and the proximity of diverticula to the orifice, and confirm the absence of mucosal inflammatory modifications and urethral patency if indicated. With the bladder empty, the cystoscope beak is positioned close to and going through the ureteric orifice. Contrast is instilled at the ureteric orifice utilizing the irrigation port of the cystoscope from a peak of 1 meter above the bladder. The bladder is emptied earlier than the process is repeated on the contralateral aspect. Rather, it should be reserved for a very select group of sufferers who pose rare, diagnostic dilemmas. Pyelonephritis propagated by reflux causes renal scarring, impedes attainment of full renal development potential, and will increase the risk for renovascular hypertension (Mattoo et al. Therefore, imaging of the higher tracts is directed at assessing renal construction and performance, with consideration to the aforementioned parameters. Reflux status, coupled with the age of the affected person, intercourse, race, family historical past of reflux, and bladder and bowel useful standing, function a information to selective imaging, which attempts to steadiness intensity of imaging research with propensity for renal damage. Indeed, in the presence of reflux, modern postnatal renal sonography provides wonderful correlation between renal length and scintigraphic hypoplasia (Farhat et al. Ultrasonography can additionally be useful for analysis of renal corticomedullary differentiation. Loss of corticomedullary differentiation, or an increase in total echogenicity of the kidney, is related to a point of renal useful impairment (Chi et al. Coupled with a comparatively smaller ipsilateral kidney, loss of corticomedullary differentiation or elevated echogenicity suggests a level of intrinsic renal dysplasia that developmentally accompanies high-grade reflux (Chi et al. Similarly, renal sonography is proscribed in its capacity to visualize minor renal cortical abnormalities. Several studies have proven the prevalence of renal scintigraphy over ultrasonography in detecting renal scars (Veenboer et al. Modern enhancements in ultrasound know-how permit imaging of perfusion abnormalities in tissue. In reflux nephropathy using color Doppler ultrasonography, renal resistive index measurements derived from blood circulate in interlobar and arcuate arteries are significantly elevated in higher grades of reflux and correlate positively with scintigraphic findings from the identical renal unit (Radmayr et al. Animal studies have also demonstrated that contrast-enhanced harmonic ultrasonography can detect histologically confirmed areas of reflux-induced pyelonephritis with great sensitivity and greater than 80% optimistic and negative predictive values (Farhat et al. The radiotracer is taken up solely by functioning proximal tubular tissue mass, the place it binds for several hours. Most institutions carry out scans using a gamma camera positioned posteriorly, nonetheless, in circumstances with severe hydronephrosis, conjugate views might measure differential function more accurately (Pippi Salle et al. Although many such affected areas in the kidney resolve, particularly with prompt medical treatment (Fern�ndez-Men�ndez et al. Ultrasonography lends itself nicely to quantitative evaluation of renal dimensions (Rodriguez et al. In reflux recognized in the neonatal interval, baseline renal dimensions are obtained, and acceptable renal progress may be monitored. This has given rise to added pressures of avoiding bladder catheterization in view of the misery it creates in young sufferers (Stashinko and Goldberger, 1998; Elder, 2005). Clinicians should resolve how every investigation, particularly invasive ones, impacts the general scientific determination tree and how the results enable the secure management of every patient, both by intervention or conservative strategies. All of this ought to be weighed against the degree of distress each test causes the child. Pinhole photographs show a traditional left kidney and a right kidney with a number of cortical defects. This strategy reconstructs three-dimensional images of the renal cortical structure, which can be seen in any aspect in 360 degrees of rotation. Despite the well-established tips for renal cortical scintigraphy from the Society of Nuclear Medicine (Mandell et al. As a common rule, the utility of scintigraphy can greatest be appreciated in the context of the information it provides related to reflux: imaging cortical defects and relative renal operate. The usefulness of this info will depend on what associated medical and radiologic information are at hand. Confirmation of acute pyelonephritis can help ensure that enough antimicrobial therapy is supplied. If surgical intervention is deliberate and vital renal asymmetry exists on ultrasonography, quantification of relative operate by scintigraphy may help within the choice between reflux correction and nephrectomy.
Discount clarithromycin 250 mg mastercard
Stents should be left four to 8 weeks on average to permit time for the healing process, coinciding with the period by which irritation decreases. All urinomas or collections have to be drained, even when the leak has ceased, and interventional radiology may be of great help placing drains. Typically, these surgical procedures require experience to tackle such accidents and surrounding tissue inflammation to obtain an optimal repair. Ureterovaginal Fistula the analysis of ureterovaginal fistula can be difficult, as this is often a delayed presentation. When the analysis is suspected, giving the patient Chapter 17 intravenous methylene blue and clamping the Foley should stain a vaginal pad blue within the presence of a fistula. In these circumstances, the presence of a vesicovaginal fistula have to be dominated out and differentiated from a ureterovaginal fistula. The double-dye pad check consists of giving the patient a load of oral pyridium while filling the bladder with methylene blue followed by clamping of the Foley catheter. An orange stain indicates a ureteral fistula, whereas blue staining is in favor of a vesicovaginal fistula. The presence of a blue stain distally and an orange stain proximally within the pad signifies concomitant presence of both fistulas. Complications of Urologic Surgery 267 Strictures Despite enough repair, stricture formation on the website of injury or fistula can happen. With the current benefits of laser and balloon dilators, endoscopic makes an attempt to manage such problems are affordable as an preliminary technique, especially for brief and nonextensive strictures. Definitive surgical restore could also be needed when the preliminary endoscopic attempt fails or the ureteral stricture is intensive and lengthy (>2 cm). It is often a difficult procedure because of ensuing fibrotic modifications within the retroperitoneum that end result from the earlier urinary leak or ureteral damage. For higher ureteral injuries, where the ends could be mobilized and approximated, a ureteroureterostomy could be tried for small segmental defects. Recently, advanced reconstructive techniques with the use a robotic platform have been described to bridge intensive gaps with buccal mucosa grafts. The appendix can also be described as an inexpensive conduit to bridge ureteral defects on the right side. One can assess the adequacy of vascular perfusion in the transected and "trimmed" ureteral ends with the Fire Fly technology of the robot. Classic techniques of ureteral reimplantation with a psoas hitch for lower ureteral defects and a Boari flap for mid-ureteral accidents may be tried robotically. Upper ureteral strictures which are intensive are at times finest managed with an ileal ureter interposition graft. Of course, open strategies for reconstruction should always be thought of when significant intraabdominal challenges exist, corresponding to multiple prior surgical procedures and adhesions that might render a robotic or laparoscopic repair not only difficult and prolonged but also at instances impossible. This ranges from preoperative stenting of the ureters to lighted stents to aid more in localization when haptic feedback is proscribed, particularly within the case of minimally invasive surgery. Often after hysterectomy, definitive restore of in depth bladder harm is the best option as the affected person would be in danger for vesicovaginal fistula formation. The commonest complication on the bladder stage at the time of urologic surgical procedure is throughout robotic radical prostatectomy, when at times a "buttonhole" defect is created on the posterior bladder lip throughout dissection of the posterior side of the vesicoprostatic junction. Care should be taken to establish the right airplane for dissection without denuding the posterior bladder neck extensively. It is essential to at all times identify the ureteral orifices when difficulty exists in dissection at this location resulting from earlier endoscopic surgery of the prostate. Temporary placement of 5-Fr pediatric feeding tubes or preoperative stenting may be necessary. Both maneuvers are helpful for the much less experienced surgeon and rarely are necessary for the skilled robotic surgeon. Another state of affairs is leakage from the site of a bladder cuff resection at the time of an open, robotic, or laparoscopic distal ureterectomy and reimplant or after an open, robotic, or laparoscopic nephroureterectomy. Management remains as outlined earlier, and determination of the leak will occur so long as the leak and bladder are adequately drained for 7 to 10 days. Urine Leaks After Radical Prostatectomy Overview Urinary leakage on the urethrovesical anastomotic junction is doubtless certainly one of the commonest issues in the early postoperative interval (days 7 to 10) reaching an incidence of 0.
Buy 250 mg clarithromycin overnight delivery
Plain radiograph of a 5-day-old infant with posterior urethral valves and bronochopulmonary dysplasia, requiring airway help, reveals reduced lung quantity and left upper and decrease lobe atelectasis. A renal ultrasound in these patients usually detects the telltale bladder wall thickening, distal ureteral dilation that requires a voiding cystourethrogram for affirmation. Sonographic picture of left kidney in a newborn identified with posterior urethral valves exhibits a big urinoma. The urinoma compresses the renal parenchyma inferiorly, and is contained inside the renal capsule. This reduced growth adversely impacts the event of the fetal pulmonary tree that requires intraluminal strain, volume, and move whereas providing mobile signaling to the developing alveoli (Husain and Hessel, 1993; Laudy et al. The remedy objective is to restore circulate of urine by way of the urethra and allow regular cyclic filling and emptying of the bladder, which is superior to urinary diversion and passive urine drainage (Smith et al. Experimental fashions corroborate medical evidence of the importance of bladder biking, and one mannequin of urinary diversion and undiversion demonstrated the adjustments that happen in a diverted bladder prevented from biking (Chun et al. A fetal sheep mannequin developed a rise in expression of extracellular matrix components and apoptosis after a excessive diversion (Chun et al. Historically, it had even been successfully carried out with a crochet hook handed retrograde into the urethra and feeling the hook catch the obstructing tissue. Innes Williams first described the engagement of valves with a hook, and Whitaker and Sherwood modified the hook by insulating the wire except for the very distal portion of the hook, which measures 6 to 7 Fr and could presumably be passed at the bedside with out basic anesthesia whereas applying a small amount of diathermy when ablating the valves (Whitaker and Sherwood, 1986). With the miniaturization of endoscopes within the age of fiberoptic and, now, digital expertise, cystoscopy could be achieved in even the smallest neonate, and endoscopic valve ablation is the preferred method at most centers right now. A wire bent on the tip and passed through a 3-Fr ureteric catheter is an alternative choice, as is the visually guided fogarty embolectomy catheter (Soliman, 2009). Valves are thin and related to minimal vascularity, and aggressive resection must be prevented. Use of a sizzling loop resectoscope for valve ablation, primarily in older kids the place a resectoscope could be readily inserted, appears to be related to a higher danger for urethral stricture, and caution must be exercised with its use (Sarhan et al. The introduction of renal ultrasonography since 1979 elevated the detection of urinomas to 15% in one research (Heikkil� et al. Forniceal rupture will seem on renal ultrasound as distorted renal parenchyma brought on by fluid trapped within the renal capsule, and transperitoneal transudation of fluid or bladder rupture will current as neonatal ascites (Greenfield et al. Although voiding cystourethrogram or radionuclide cystography may delineate the positioning of leakage for ascites, the cause is often tough to decide (Patil et al. It is only in circumstances during which the ascites is causing respiratory misery, severe abdominal distension, or other medical symptoms that percutaneous drainage or tapping ascites becomes needed, however these interventions are unusual. There is some debate as to whether or not a urinoma heralds better or worse renal perform for the affected side. Numerous research have postulated that the urinoma serves as a pop-off mechanism, thereby lowering renal dysplasia on a given aspect, and others show globally preserved renal operate, including an index of long-term renal severity (Rittenberg et al. Others maintain that the urinoma, especially one retained inside the renal capsule and compressing the kidney, impairs ipsilateral renal perform and is a harbinger for worsened renal prognosis or has no bearing at all on long-term renal perform (Patil et al. Up to 64% of these children had a normal prenatal ultrasound, and most introduced with urinary tract infections, voiding complaints, and acute renal failure in 10% (Engel et al. A voiding cystourethrogram have to be repeated after valve ablation inside 1 month to make certain that the valves are not seen. Bladder neck hypertrophy and the following elevation of the bladder neck proximal to the posterior urethra, together with the unfinished emptying that appears to persist on imaging in some boys after valve ablation, prompted an interest in transurethral incision of the bladder neck during or after main valve ablation. The earliest stories of procedures to handle this bladder neck hypertrophy included a Y-V plasty and bladder neck incision (Bauer et al. Still, the concept of bladder neck obstruction and bladder neck incision continues to be supplied as a surgical option (Androulakakis et al. Although some research affirm that the bladder neck incision advantages emptying in kids with a neurogenic bladder, the considerations of retrograde ejaculation and lack of improvement compared with controls in even short-term pilot studies have restricted the adoption of this system (Christensen et al. There is a dearth of studies from a number of establishments confirming the extended durability and advantage of bladder neck incision. One long-term study restricted to 21 patients older than 18 years of age who underwent bladder neck incision in infancy reported no incontinence in maturity and an absence of great ejaculatory dysfunction (Keihani et al. The vesicostomy does scale back bladder storage pressures and may optimize glomerular filtration price in some circumstances (Kim et al. The argument that the vesicostomy defunctionalizes the bladder and results in decreased compliance in the long term has been refuted, as a properly created vesicostomy permits bladder filling Chapter 33 and preserves contractile function as urine should be expulsed through the stoma, albeit at a reduced leak point pressure (Hutcheson et al. The vesicostomy is classically created with a 2-cm midline transverse incision made halfway between the pubic symphysis and the umbilicus.
Cheap clarithromycin online mastercard
Excessive length of the extravesical limb could make such dilation more problematic. Ileocecal Valve Use of the ileocecal valve as a continence mechanism started with Gilchrist et al. In basic, a brief section of terminal ileum, whether imbricated or tailor-made, is used as an efferent limb. This phase should be stored as brief and straight as potential to facilitate easy intermittent catheterization. Continence is based on the imbricated ileocecal valve, not the size of the efferent limb. The imbrication is usually secured with interrupted, permanent sutures, involving the very distal ileum and ileocecal valve, and the imbrication is carried onto the cecum. Besides the appendix, this continence mechanism is probably the simplest and has the shortest learning curve to achieve reliable outcomes. Continence charges have been reported as high as 95% with preservation of normal higher tracts (Hensle and Ring, 1991; Kaefer et al. Initial incision may be made to one aspect to form a shorter limb for implantation within the bladder and an extended one to be introduced via the abdominal wall. They famous a very low incidence of detrimental effect on gastrointestinal function in a choose group of patients with neurogenic dysfunction. Urine from the reservoir and generated stress is allowed to enter a sleeve of ileum around the catheterizable channel. Compression of the internal tube theoretically offers continence, and early expertise was encouraging. Initial continence rates approached 75% after which 90% with a single revision (Benchekroun et al. Others have been unable to duplicate Continent Vesicostomy Yachia (1997) described creation of a bladder tube fashioned from a large flap of the anterior bladder wall. An try and present a continence mechanism was fashioned by weaving the bladder tube by way of the rectus muscle for compression and continence. Continence of their small, short-term series was reported to be 100 percent, but this has not been duplicated. A rectangular flap in continuity with the bladder is tubularized over a 14-Fr to 16-Fr catheter. The bladder is plicated around the proximal 3 cm of the tube using nonabsorbable suture to create a type of nipple much like gastric fundoplication. Macedo and Srougi (2000) described an analogous continence mechanism created at the time of preliminary augmentation. Their technique is doubtlessly appealing for sufferers requiring augmentation and having no appendix because of the simplicity; however, continence is based on a kind of nipple valve that traditionally has been troublesome to keep fastened. Casale (1991) has described a type of continent vesicostomy during which the continence mechanism is based on a flap valve created from a tubularized strip of bladder mucosa. Parallel incisions 3 cm aside are made into the anterior bladder and used to create a protracted rectangular flap. The stomach wall must be measured to make positive that the strip is lengthy sufficient to attain the pores and skin with out pressure. The muscle portion is left broad to come around with out rigidity and provide good blood provide. The edges of this strip are mobilized till it can be tubularized along its entire length. It could also be beneficial to mobilize just one edge over to the other aspect to avoid overlapping suture traces. Casale (1991) originally incised the mucosa transversely on the end of the intravesical strip to be tubularized; Rink et al. The bladder mucosa from either aspect of the channel is then mobilized and closed over the mucosal tube to create a flap valve. More extensive mobilization of the side reverse that mobilized for the inner tube allows closure without overlapping suture lines, which may help avoid fistula formation and incontinence.
Order 250 mg clarithromycin with amex
Novljan G, Kenig A, Rus R, et al: Cyclic voiding urosonography in detecting vesicoureteral reflux in youngsters, Pediatr Radiol 18(10):992�995, 2003. Oswald J, Schwentner C, Brenner E, et al: Extracellular matrix degradation and lowered nerve supply in refluxing ureteral endings, J Urol 172(3):1099� 1102, 2004. Phan V, Traubici J, Hershenfield B, et al: Vesicoureteral reflux in infants with isolated antenatal hydronephrosis, Pediatr Nephrol 18(12):1224�1228, 2003. Pietrzak-Stelasiak E, Biekiewicz M, Wonicki W, et al: Usefulness of parametric renal clearance pictures within the assessment of primary threat elements for renalnal clearance pictures in the assessment of fundamental risk factors for renal scarring in youngsters with recurrent urinary tract infections, Nucl Med Rev Cent East Eur 20(2):76�80, 2017. Piskunowicz M, wito D, Rybczyska D, et al: Comparison of voiding cystourethrography and urosonography with second-generation distinction brokers in simultaneous potential study, J Ultrason 16(67):339�347, 2016. Polito C, La Manna A, Capacchione A: Height and weight in youngsters with vesicoureteric reflux and renal scarring, Pediatr Nephrol 10(5):564�567, 1996. Polito C, Marte A, Zamparelli M, et al: Catch-up progress in children with vesico-ureteric reflux, Pediatr Nephrol 11(2):164�168, 1997. Preda I, Jodal U, Sixt R, et al: Normal dimercaptosuccinic acid scintigraphy makes voiding cystourethrography unnecessary after urinary tract infection, J Pediatr 151(6):581�584, 584. Radmayr C, Klauser A, Maneschg C, et al: Importance of the renal resistive index in children affected by vesicoureteral reflux, Eur Urol 36(1):75�79, 1999. Reid G, Devillard E: Probiotics for mother and youngster, J Clin Gastroenterol 38(Suppl 2):S94�S101, 2004. Riccabona M, Ring E, Maurer U: Scintigraphy and sonography in reflux nephropathy: a comparison, Nucl Med Commun 14(4):339�342, 1993. Roussey-Kesler G, Gadjos V, Idres N, et al: Antibiotic prophylaxis for the prevention of recurrent urinary tract infection in youngsters with low grade vesicoureteral reflux: results from a prospective randomized study, J Urol 179(2):674�679, discussion 679, 2008. The voiding cystourethrogram experience of young youngsters, Issues Compr Pediatr Nurs 21(2):85�96, 1998. Stokland E, Andr�asson S, Jacobsson B: Sedation with midazolam for voiding cystourethrography in kids: a randomised double-blind examine, Pediatr Radiol 33(4):247�249, 2003. Taskinen S, Heikkil� J, Rintala R: Effects of posterior urethral valves on long-term bladder and sexual function, Nat Rev Urol 9(12):699�706, 2012. Taylor A Jr: Quantitation of renal perform with static imaging agents, Semin Nucl Med 12(4):330�344, 1982. Uetani N, Bouchard M: Plumbing within the embryo: developmental defects of the urinary tracts, Clin Genet 75(4):307�317, 2009. Walker D, Richard G, Dobson D, et al: Maximum urine focus: early means of identifying patients with reflux who may require surgery, Urology 1(4):343�346, 1973. Salvini F, Granieri L, Gemmellaro L, et al: Probiotics, prebiotics and child health: where are we going Sanna-Cherchi S, Reese A, Hensle T, et al: Familial vesicoureteral reflux: testing replication of linkage in seven new multigenerational kindreds, J Am Soc Nephrol 16(6):1781�1787, 2005. Seruca H: Vesicoureteral reflux and voiding dysfunction: a potential study, J Urol 142(2 Pt 2):494�498, dialogue 501, 1989. Shafik A: Electroureterogram within the obstructed ureter and vesicoureteral reflux, J Surg Res 65(2):145�148, 1996. Shaikh N, Hoberman A, Keren R, et al: Recurrent urinary tract infections in youngsters with bladder and bowel dysfunction, Pediatrics 137(1):2016a. Sj�str�m S, Sill�n U, Bachelard M, et al: Spontaneous decision of high grade infantile vesicoureteral reflux, J Urol 172(2):694�698, discussion 699, 2004. Smellie J, Edwards D, Hunter N, et al: Vesico-ureteric reflux and renal scarring, Kidney Int Suppl 4:S65�S72, 1975. Snodgrass W: Relationship of voiding dysfunction to urinary tract an infection and vesicoureteral reflux in children, Urology 38(4):341�344, 1991. S�rensen K, Lose G, Nathan E: Urinary tract infections and diurnal incontinence in women, Eur J Pediatr 148(2):146�147, 1988. Wallin L, Bajc M: the importance of vesicoureteric reflux on kidney improvement assessed by dimercaptosuccinate renal scintigraphy, Br J Urol 73(6):607�611, 1994.
Order clarithromycin 250mg visa
The secretory nature of gastric mucosa could at times be detrimental to the affected person and can lead to two distinctive complications of gastrocystoplasty. Episodes of hypokalemic, hypochloremic metabolic alkalosis after acute gastrointestinal diseases had been famous in 5 of 37 sufferers after gastrocystoplasty (Hollensbe et al. The episodes were vital enough to require hospitalization in all sufferers and had been recurrent in 2 sufferers. Patients with the primary indication for consideration of gastrocystoplasty could be the ones at best risk for this unusual complication. It has been proposed that the alkalosis results from ongoing chloride loss from the gastric section in the bladder within the face of decreased oral consumption. One affected person of their series eventually required resection of three quarters of the gastric section in the bladder due to recurrent problems with alkalosis, and several required remedy with H2 blockers or H+/K+ ion pump inhibitors. All sufferers and families should be made aware of this potential problem because it has been reported to happen intermittently in 3% to 24% of sufferers. A composite reservoir of abdomen and ileum or colon might present a more metabolically neutral reservoir (Austin et al. Acid secretion by gastric mucosa may end in one other distinctive downside after gastrocystoplasty, the hematuria-dysuria syndrome. Almost all sufferers after gastrocystoplasty with regular sensation have occasional hematuria or dysuria with voiding or catheterization beyond what is anticipated with different intestinal segments (Leonard et al. Others have noted a similar requirement for short-term and continual medical therapy (Adams et al. The signs of the hematuria-dysuria syndrome do respond nicely to H2 blockers and hydrogen ion pump blockers. The indicators and symptoms of the hematuria-dysuria syndrome are more than likely secondary to acid irritation. Work has instructed that Helicobacter pylori might play a task on this complication (Celayir et al. Leong first noted glanular excoriation after gastrocystoplasty in a patient with voiding symptoms (Ngan et al. It is imperative to obtain dependable urinary continence in patients undergoing gastrocystoplasty as a outcome of urinary leakage might outcome in the exposure of the skin to gastric secretions and in gastric secretions which are poorly diluted. They evaluated the affect of urine on gastrocystoplasties in dogs (Castro-Diaz et al. The animals developed marked inflammation of the gastric segment and native bladder after creation of a dry gastrocystoplasty; three of 9 canine developed ulceration and perforation. Use of H2 blockers resulted in some protection for the animals; nonetheless, such a medical scenario should certainly be prevented. Rare perforations and ulcerations have been noted clinically with out defunctionalization (El-Ghoneimi et al. Chapter 37 Lower Urinary Tract Reconstruction in Children 699 Urinary Tract Infection Bacteriuria is widespread after intestinal cystoplasty, significantly in sufferers requiring intermittent catheterization (Gearhart et al. Bacteriuria has been noted even when sufferers are maintained on day by day oral antibiotics or antibiotic irrigation (Casale et al. The incidence of symptomatic cystitis after cystoplasty probably is dependent upon the length of follow-up and the diligence with which signs are sought. All patients and families ought to be told to count on some indicators or symptoms of cystitis. Recurrent episodes of symptomatic cystitis requiring treatment occurred in 23% of sufferers after ileocystoplasty, 17% of patients after sigmoid cystoplasty, 13% after cecocystoplasty, and 8% after gastrocystoplasty at Indiana University (Hollensbe et al. The similar trend among different bowel segments was noted for febrile infections, although there was no statistically important distinction among the varied segments. The incidence of pyelonephritis after augmentation cystoplasty, as lengthy as higher tract issues are corrected, is just like that noted for conduit diversion, whether refluxing or not (McDougal, 1992b). Infections might often be more problematic in an immunocompromised affected person (Alfrey et al. Bacteriuria must be treated in the presence of serious signs such as incontinence or suprapubic ache and may be treated if hematuria, foul-smelling urine, or remarkably elevated mucus production happens. Bacteriuria should be handled if the urine culture demonstrates development of a urea-splitting organism that will result in stone formation.
Discount clarithromycin 500mg
More in-depth dialogue of clinical entities may be found elsewhere on this text but are mentioned briefly here for context. Voiding Symptoms In boys, historical past of deviated or narrowed urinary stream, prolonged urination, inability to utterly empty, straining, dysuria, and postvoid dribbling ought to be elicited. Sitting with legs tightly collectively, slouching, or sitting on the edge of the toilet with ft barely touching the floor promotes pelvic flooring musculature activation, which increases bladder outlet resistance. This could result in increased voiding pressures and contribute to dysuria or incomplete emptying, subsequently growing the danger for bladder dysfunction or urinary tract infections. Sometimes, the kid might be encouraged to sit on the toilet "backwards" going through the tank, thus making certain the legs are apart to decrease poor posture. Posturing maneuvers improve perineal strain and inhibit bladder contractions through the sacral reflex arc, probably via increased afferent cosignaling (gate management principle of ache transmission, which states that increased large-fiber afferent alerts will decrease alerts transmitted by smaller fibers by way of the dorsal horn). The method to working up decrease urinary tract symptoms contains first attempting to determine an anatomic or neurologic etiology for lower urinary tract symptoms. The important components of a whole historical past ought to embrace symptomatology, voiding frequency, bowel function, prior urinary tract infections, relevant family historical past, maternal prenatal historical past including screening ultrasonography, delivery history, developmental milestones including bathroom coaching, neuropsychiatric circumstances, past medical and surgical history, social historical past, diet, and review of methods. Bowel Function Bowel dysfunction is often coincident with lower urinary tract dysfunction given related innervation of the rectum via the sacral nerve roots (S2�S4) (Burgers et al. As such, obtaining bowel perform history is extremely important, as there are instances by which predominant bowel dysfunction will be the only underlying reason for urinary signs. Specificity when obtaining a bowel perform historical past is essential because constipation as an idea confuses many parents and sufferers. Asking if a patient has constipation is normally insufficient, so we advise suppliers delve more specifically into bowel movement frequency, fecal incontinence, belly ache, size of stool, and consistency of bowel actions in accordance with the Bristol stool scale (Lewis and Heaton, 1997). Sometimes referred to within the United Kingdom because the "Meyers scale," it was developed at the University of Bristol in 1997 (Lewis and Heaton, 1997). The scale ranges from 1 to 7, with 1 comparable to small, Storage Symptoms the urologist ought to ask about signs attributable to lower urinary tract storage dysfunction such as urgency, frequency, or incontinence. Incontinence timing must be decided (continuous versus intermittent, day versus evening, how often). Signs of elevated or decreased bladder capacity may also be inferred from the history, and a directed workup to verify this might be helpful. Secondary enuresis (new incontinence after at least 6 months of being dry) could occur in response to adjustments in every day actions or new stressors at house or school. Diet also needs to be reviewed with the patient, as known bladder irritants like caffeinated beverages. Avoid dangling ft over edge as this likely increases pelvic floor muscle tone, inhibiting relaxation for voiding. This scale supplies a useful, objective reference for documenting stool consistency when talking to patients about bowel operate. However, the definition of functional constipation and/or bowel dysfunction stays controversial (Austin et al. Clinical Aids Patients diaries can be particularly helpful in determining elimination habits, and corresponding urinary symptoms. The 7-day bowel and bladder diary involves the affected person or father or mother monitoring timing of voids, bowel actions, associated stool consistency, and presence of any incontinence of urine or stool in the day or night time. This device supplies a really full picture, eliminating problems with recall bias (Lane et al. Objective information concerning bowel function can assist with the prognosis of practical constipation. For sufferers with a main grievance of voiding dysfunction, a 48-hour frequency-volume chart may be obtained (Hoebeke et al. A rest room seat "hat" with measurements or graduated cylinder should be offered to measure volumes. Weekends with regular deliberate activities are instructed to full the duty, which consists of recording volumes of fluid consumption and output and paying attention to any incontinence episodes. This kind of diary may help decide hard pellets and 7 similar to watery diarrhea. We use it as a clinical communication assist with our patients and their families when it comes to what to try for and to facilitate titration of supplemental fiber or laxatives.
Purchase clarithromycin 250 mg online
These lower-pole arteries cross ventral to the ureter and can cause intermittent ureteropelvic junction obstruction requiring repositioning of the ureter behind the accent lower-pole renal artery. The common variation in blood supply to the kidney is a mirrored image of the continually altering embryonic renal vasculature. This is reflected in that 25% of adult kidneys have two or more renal arteries (Moore et al. Clinical Correlation: Multicystic Dysplastic Kidneys Multicystic dysplastic kidneys occur in approximately 1: 2400 to 1: 4800 newborns. In the majority of cases, this could be a unilateral process with the nonaffected kidney exhibiting compensatory hypertrophy (Gaither et al. Multicystic dysplastic kidneys are characterised by nonfunctional renal tissue with out recognizable glomeruli. The inferior poles of the kidneys can also fuse, forming a horseshoe kidney (incidence ~1: 500) that crosses ventral to the aorta. Typically, the horseshoe kidney produces no symptoms however may be related to a slight increase in ureteropelvicjunction obstruction and renal calculi. Rarely, the kidney fuses to the contralateral one and ascends to the alternative facet, resulting in a cross-fused ectopy. With the formation of mesonephric ducts, embryonic kidneys develop sequentially within the order of pronephros (completely reabsorbed), mesonephros (partially reabsorbed), and metanephros (permanent kidney). The final pair of arteries varieties in the upper lumbar area and becomes the definitive renal arteries. Clinical Correlation: Cystic Renal Disease Autosomal recessive polycystic kidney illness occurs in roughly 1: 20,000 stay births. The extreme renal illness often leads to pulmonary hypoplasia causing neonatal dying. Isaacson D, Shen J, Overland M, et al: Three-dimensional imaging of the creating human fetal lower urogenital-genital tract: detached stage to female and male differentiation, Differentiation 103:14�23, 2018. Treatment include documenting that the contralateral kidney stays healthy and compensates for the shortage of function of the multicystic dysplastic kidney. Renal agenesis may be a nonrecognizable form of multicystic dysplastic kidney by which the involution occurs early in gestation before the abnormal renal growth may be detected by prenatal sonogram. Aboseif S, El-Sakka A, Young P, et al: Mesenchymal reprogramming of grownup human epithelial differentiation, Differentiation 65(2):113�118, 1999. Aumuller G, Riva A: Morphology and functions of the human seminal vesicle, Andrologia 24(4):183�196, 1992. Baskin L, Meaney D, Landsman A, et al: Bovine bladder compliance increases with normal fetal improvement, J Urol 152(2 Pt 2):692�695, dialogue 696�697, 1994. Baskin L, Shen J, Sinclair A, et al: Development of the human penis and clitoris, Differentiation 103:74�85, 2018. Batourina E, Gim S, Bello N, et al: Vitamin A controls epithelial/mesenchymal interactions via Ret expression, Nat Genet 27(1):74�78, 2001. Batourina E, Tsai S, Lambert S, et al: Apoptosis induced by vitamin A signaling is crucial for connecting the ureters to the bladder, Nat Genet 37(10):1082� 1089, 2005. Beaudoin S, Simon L, Bargy F: Anatomical foundation of a common embryological origin for epispadias and bladder or cloacal exstrophies, Surg Radiol Anat 19(1):11�16, 1997. Capito C, Echaieb A, Lortat-Jacob S, et al: Pitfalls within the diagnosis and administration of obstructive uterovaginal duplication: a sequence of 32 cases, Pediatrics 122(4):e891�e897, 2008. Cebrian C, Borodo K, Charles N, et al: Morphometric index of the creating murine kidney, Dev Dyn 231(3):601�608, 2004. Chandar J, Garcia J, Jorge L, et al: Transplantation in autosomal recessive polycystic kidney disease: liver and/or kidney Hayashi N, Sugimura Y, Kawamura J, et al: Morphological and useful heterogeneity in the rat prostatic gland, Biol Reprod 45:308�321, 1991. Herzlinger D, Koseki C, Mikawa T, et al: Metanephric mesenchyme contains multipotent stem cells whose destiny is restricted after induction, Development 114(3):565�572, 1992. Herzlinger D, Qiao J, Cohen D, et al: Induction of kidney epithelial morphogenesis by cells expressing Wnt-1, Dev Biol 166(2):815�818, 1994. Isaacson D, Shen J, Overland M, et al: Three-dimensional imaging of the developing human fetal urogenital-genital tract: Indifferent stage to male and female differentiation, Differentiation 103:14�23, 2018. Jost A: Problems of fetal endocrinology: the gonadal and hypophyseal hormones, Rec Prog Horm Res eight:379�418, 1953.
References
- Domaingue CM, Nye DH. Hypotensive effect of mannitol administered rapidly. Anaesth Intensive Care. 1985;13:134-136.
- Mollen RM, Kuijpers JH, van Hoek F. Effects of rectal mobilization and lateral ligaments division on colonic and anorectal function. Dis Colon Rectum 2000;43(9):1283-87.
- Amanzio M, Pollo A, Maggi G, Benedetti F. Response variability to analgesics: a role for non-specific activation of endogenous opioids. Pain. 2001;90(3):205-215.
- Nick WV, Zollinger RW, Pace WG. Retroperitoneal hemorrhage after blunt abdominal trauma. J Trauma. 1967;7(5):652-659.
- McPherson ME, Kelly H, Patel MS, et al. Persistent risk of tuberculosis in migrants a decade after arrival in Australia. Med J Aust 2008; 188: 528-531.
- Hotchkiss RS, Levy JH, Levi M. Sepsis-induced disseminated intravascular coagulation, symmetrical peripheral gangrene, and amputations. Crit Care Med. 2013;41(10):e290-e291.
- Remmler D, Denny A, Gosain A, Subichin S. Role of threedimensional computed tomography in the assessment of nasoorbitoethmoidal fractures. Ann Plast Surg 2000;44:553-562.