
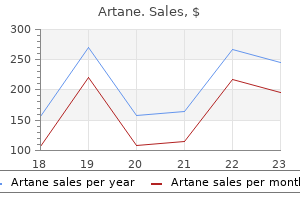
Artane dosages: 2 mg
Artane packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Cheapest artane
It is synthesized by respiratory epithelial cells, serous glandular cells, and macrophages. Decreased levels of lysozyme have been correlated with elevated susceptibility to acute bronchitis. Lactoferrin acts to agglutinate and kill bacteria, improve neutrophil adherence, and prime neutrophil superoxide manufacturing. Its name derives from the fact that lactoferrin also capabilities to block iron from supporting bacterial metabolism. Lactoferrin binds to micro organism by way of the recognition of highly conserved carbohydrate moieties on the microbial cell surface. Defensins are a household of small proteins with intrinsic antimicrobial exercise that are discovered within the lung and on other mucosal surfaces, including the gastrointestinal and reproductive tracts. Defensins have broad antimicrobial activity towards both gram-positive and gram-negative organisms. They act by making the microbial cell wall permeable, thus inflicting launch of microbial cell contents and destruction of the membrane potential. Their antimicrobial operate is a result of binding and aggregating microbes and facilitating interaction with phagocytic cells. They also seem to be important in the regulation of pulmonary macrophage exercise and cytokine production. Animal models point out that defects in both of these proteins increase the susceptibility to respiratory an infection; nonetheless, human illness related to a genetic mutation or deletion has not been recognized. These cells constitute a major form of protection in opposition to materials that has escaped deposition in the higher airway and has reached the intrathoracic airways or the alveolar structures. Pulmonary alveolar macrophages are massive cell cells approximately 15 to 50 �m in diameter. Their cytoplasm incorporates quite lots of Lung Defense Mechanisms n 289 granules of assorted styles and sizes, lots of which are packages of digestive enzymes that may dispose of ingested overseas material. Alveolar macrophages have a major role in killing microorganisms that have reached the lower respiratory tract. They additionally release chemoattractant cytokines (chemokines) that recruit different inflammatory cells. When an alveolar macrophage is exposed to inhaled particles or micro organism, attachment of the foreign materials to the surface of the macrophage is step one within the processing sequence. The particles or bacteria are engulfed inside the plasma membrane, which invaginates and pinches off inside the cell to form a cytoplasmic phagosome containing the now isolated foreign material. In some circumstances, this sequence of attachment and phagocytosis is facilitated by opsonins, which coat the international material. Opsonins are proteins that bind to extracellular supplies and make them extra adherent to phagocytic cells and more amenable to engulfment or ingestion. Opsonins can be particular for the particular overseas substance, corresponding to antibodies directed in opposition to antigenic material, or they might show nonspecific binding to quite a lot of substances. Particularly essential specific opsonins are antibodies of the IgG class directed against antigenic international materials, either bacteria or different antigenic particles. Nonspecific opsonins within the lung embody secretory IgA, complement, and fibronectin. After micro organism or different overseas materials is isolated inside phagosomes, a means of intracellular digestion happens throughout the macrophage. Often the phagosomes combine with lysosomes to form phagolysosomes, during which proteolytic enzymes equipped by the lysosome digest, detoxify, or destroy the phagosomal contents. In addition to lysosomal enzymes, quite a lot of oxidation merchandise, such as hydrogen peroxide and other intermediate merchandise of oxidative metabolism, are poisonous to micro organism and play a job in the ability of the macrophage to kill ingested microorganisms. Macrophages release inflammatory mediators such as tumor necrosis factor- and interleukin-1, as well as other cytokines and chemokines that are energetic in recruiting extra inflammatory cells. In some circumstances, similar to with inhaled silica particles, the ingested material is poisonous to the macrophage and finally may kill the phagocytic cell.
Syndromes
- A family history of inherited colorectal cancer syndromes, such as familial adenomatous polyposis (FAP) or hereditary nonpolyposis colorectal cancer (HNPCC)
- Lupus nephritis
- Infection of the scrotal sac
- Emphysema
- Irregular, fast heart rhythms (arrhythmias)
- Sun-related changes of older skin
Cheap 2mg artane
Only when a transection is made between the medulla and the spinal wire does ventilation cease, indicating that the respiratory generator resides within the medulla. In humans and other mammals, the gathering of neurons in the ventrolateral medulla that seems to be important for respiratory pattern generation is termed the pre-B�tzinger advanced. Although the respiratory center (or generator) has been referred to as a single region, a couple of community of neurons within the medulla may be concerned in initiating and coordinating respiratory activity. According to a preferred model, one group of neurons is liable for initiating inspiration and regulating its speed as a outcome of the intensity of neuronal activity; one other group of neurons controls "switching off " inspiration and therefore determines the onset of expiration. Therefore, there are two aspects of ventilatory control: (1) the degree of inspiratory drive or central inspiratory activity (which regulates the inspiratory circulate rate), and (2) the timing mechanism (which controls the termination of inspiration). These two figuring out components act in live performance to set the respiratory fee and tidal volume and thus the minute air flow and specific pattern of respiratory. For instance, enter from the pons appears to be needed for a traditional, coordinated respiratory pattern. When the affect of the pons is misplaced, irregularities within the respiratory pattern ensue. In addition to pathways involved in the "automatic" or involuntary control of ventilation, the cerebral cortex exerts a conscious or voluntary control over ventilation. Cortical overriding of computerized management could be seen with either voluntary breath holding or hyperventilation. Interestingly, the automated control of ventilation could additionally be disturbed while acutely aware control stays intact. In these cases, during wakefulness the cerebral cortex exerts adequate voluntary control over air flow to preserve normal arterial blood gas values. Further analysis into the pathogenesis of this condition undoubtedly will result in higher understanding of the mechanisms of normal ventilatory control. Elevation of Pco2 (hypercapnia) and depression of Po2 (hypoxemia) will both stimulate air flow. In each case, one or more chemoreceptors detect alterations in Pco2 or Po2 and accordingly range their input to the medullary respiratory middle. A central respiratory generator inside the medulla controls activity of the respiratory muscular tissues. The carotid chemoreceptors, that are quantitatively far more necessary than the aortic chemoreceptors, are located simply beyond the bifurcation of each frequent carotid artery into the interior and exterior carotid branches. The aortic chemoreceptor is found between the pulmonary artery and the aortic arch. These chemoreceptors are sensitive to adjustments in Po2, with hypoxia stimulating chemoreceptor discharge. In adults, the peripheral carotid physique chemoreceptors also have a role in sensing Pco2. Under normoxic conditions, the peripheral chemoreceptors are a lot much less essential than the central chemoreceptors for maintaining Pco2. However, arterial hypoxemia increases the sensitivity of the peripheral Pco2 receptors, so if hypoxemia and hypercarbia are each current, the carotid body chemoreceptor might be maximally stimulated to increase ventilation. The information in the end is transmitted to the medullary respiratory heart so that its output is augmented. Stretch receptors positioned inside the clean muscle of airway walls reply to changes in lung inflation. In diving animals, this stretch receptor reflex (the Hering-Breuer reflex) is answerable for apnea that happens as a end result of lung inflation. Presumably, stretch receptors contribute to switching off inspiration and initiating expiration after a crucial degree of inspiratory inflation has been reached. Anatomic and Physiologic Aspects of Neural, Muscular, and Chest Wall Interactions with the Lungs n 233 or irritating mud. Juxtacapillary (or J) receptors are discovered throughout the pulmonary interstitium, adjacent to capillaries. One of their results is to cause tachypnea, and so they could additionally be responsible for the respiratory stimulation brought on by inflammatory processes or accumulation of fluid inside the pulmonary interstitium. Receptors in the chest wall, notably in the intercostal muscle tissue, appear to play a task in fine-tuning air flow. The muscle spindles are part of a reflex arc that adjusts the output of respiratory muscles if the desired diploma of muscular work has not been achieved.
Artane 2 mg with visa
The role of high-resolution computed tomography within the work-up of interstitial lung disease. The scientific utility of bronchoalveolar lavage in diffuse parenchymal lung illness. The common ideas mentioned in Chapter 9 apply to most of these situations, and the options emphasized here are these peculiar to or characteristic of each cause. Considering the huge number of diffuse parenchymal lung diseases, this chapter solely scratches the surface of data out there. Examples of the many responsible brokers embody silica, asbestos, coal, talc, mica, aluminum, and beryllium. In most cases, exposure has occurred for a chronic time because of occupational components. In a few of these ailments the parenchymal course of progresses even within the absence of continued exposure. For an inhaled inorganic mud to provoke damage to the lung parenchyma, it should be deposited at an applicable space of the lower respiratory tract. If particle size is merely too large or too small, deposition tends to be within the upper airway or within the bigger airways of the tracheobronchial tree. Abstract A number of known etiologic brokers could cause diffuse parenchymal lung illness, also referred to as interstitial lung disease. These embody inorganic dusts (the pneumoconioses), organic antigens (the reason for hypersensitivity pneumonitis), medicine, and radiation to the thorax. Some of these disorders involve toxicity to , or activation of macrophages, whereas beryllium induces a hypersensitivity reaction that clinically mimics sarcoidosis. Many organic antigens can induce a hypersensitivity pneumonitis, which can have a presentation starting from an acute sickness with transient pulmonary infiltrates to a continual diffuse parenchymal lung illness. A big selection of medication at the moment are known to be associated with parenchymal lung disease, with an important classes being most cancers chemotherapeutic agents and a selection of newer biological medicine, but a quantity of other miscellaneous medication have additionally been implicated. Finally, radiation therapy directed to the thorax, most commonly for breast cancer, lung most cancers, or Hodgkin illness, could be related to an acute inflammatory course of in the lungs (radiation pneumonitis) or a extra continual fibrotic process (radiation fibrosis). Keywords Occupational lung illness Pneumoconiosis Silicosis Asbestosis Berylliosis Hypersensitivity pneumonitis Drug-induced lung disease Radiation-induced lung disease 146 n Principles of Pulmonary Medicine No effective therapy is out there for parenchymal lung disease caused by most inhaled inorganic dusts. Therefore the essential issues dealing with physicians are recognition and prevention of these problems. Total avoidance of publicity is the optimum form of prevention, however when publicity is critical, appropriate precautions with effective masks or respirators are essential. For details about the numerous different agents, seek the assistance of the more detailed references at the finish of this chapter. Silicosis Silicosis is the diffuse parenchymal lung illness resulting from exposure to silica (silicon dioxide). Of several crystalline forms of silica, quartz is the one most regularly encountered, often as a component of rock or sand. Persons at risk embody sandblasters, onerous rock miners, quarry staff, and stonecutters. However, with significantly heavy doses of inhaled silica, as are present in sandblasters, an acute type of the illness may occur with much shorter durations of exposure. The presumed pathogenetic impact of silica has centered around its potential toxicity for macrophages. Silica particles in the decrease respiratory tract are phagocytosed by pulmonary macrophages. Freshly reduce silica particles are extra pathogenic than older particles, doubtless as a end result of the freshly minimize floor is very reactive and generates extra reactive oxygen species. Phagocytosis of silica particles leads to apoptotic cell dying, release of the toxic silica particles, and a repeat of the method after the particles are reingested by different macrophages. With each cycle of activation and destruction, the macrophages release chemical mediators that provoke or perpetuate an alveolitis, ultimately leading to development of fibrosis. Pathologically, the inflammatory process initially is localized around the respiratory bronchioles however ultimately becomes more diffuse throughout the parenchyma. Silicotic nodules are believed to be areas in which the cycle of macrophage ingestion, activation and destruction and release of the toxic silica particles occurs. The most common radiographic appearance of silicosis is notable for small, rounded opacities or nodules.

Buy artane 2 mg visa
The posterior portion of the vulva is equipped by the pudendal nerve and by the posterior cutaneous nerve of the thigh. The clitoris and the vestibule also receive parasympathetic innervation from the cavernous nerves, derived from the uterovaginal plexus. Areas of anatomic dissection within the feminine pelvis the areas of dissection in the female pelvis relevant to the gynecologic surgeon are the presacral house, the pelvic brim, the pelvic sidewall, the base of the broad ligament/ base of the cardinal ligament, the paravesical house, the retropubic house, the vesicovaginal area, the pararectal space, and the rectovaginal house. The paravesical (paravaginal), vesicovaginal, and rectovaginal areas are mentioned from both the intrapelvic route and the intravaginal route. Mention of surgical dissections in each of these areas refers to the dissection techniques already discussed. The presacral area the presacral space is the area of surgical dissection and performance of the "presacral neurectomy" for ladies with "central" persistent pelvic ache, extreme dysmenorrhea, and proven endometriosis. This potential house is bordered superiorly by the bifurcation of the aorta at the level of the fourth lumbar vertebra and inferiorly by the promontory of the first sacral vertebra. Laterally to the right travels the right frequent iliac artery and proper ureter, whereas on the left programs the left widespread iliac vein and left ureter. Posteriorly, the center sacral artery (from the aorta) and a plexus of fragile veins on the anterior longitudinal ligament are found. Between the peritoneum and the posterior border of the presacral area, a number of fused sheets of visceral connective tissue enveloping the a quantity of visceral nerves coursing via this area are discovered. These nerves emanate from preaortic ganglia and ultimately enter into the right and left hypogastric nerves (Video 1. These presacral nerves, or visceral nerves of the superior hypogastric plexus, are very nice or invisible to the bare eye. They are enveloped in and obscured by the fatty areolar tissue throughout the sheets of visceral connective tissue. The presacral plexus forms a geometrical webbing, which could be very variable in location, formation, and size. Dissection must utilize the tenting of tissues as nicely as light traction and countertraction to thin out the several layers of visceral connective tissues to see the bigger structures bordering this space while lifting the visceral connective tissues away from very vascular posterior border. Remember, these fine nerves can solely be seen if some of the nerves have bodily coalesced together. Even then, some or many nerves is in all probability not removed for the reason that bulk of the plexus could cross laterally to the left, as famous. The pelvic brim this is the realm more than likely to be untouched by endometriosis, ovarian remnant presence, infection, and subsequent scarring and adhesion formation. Therefore, this is the realm most ideally suited to begin a retroperitoneal sidewall dissection to find a way to find the ureter and major blood vessels coming into into the pelvis. The structures of the pelvic brim enter into the pelvis, one over another in a vertical orientation, and then rotate 90� to kind the three surgical layers of the pelvic sidewall (Video 1. The parietal peritoneum covers the ovarian vessels within the infundibulopelvic ligament, which course over the ureter, that, in turn, passes over the bifurcation of the widespread iliac artery located at the pelvic brim overlying the sacroiliac joint. The first layer, the ureteral layer, is the ureter and its surrounding visceral connective tissue sheath attached to the parietal peritoneum. The second, the visceral layer, is the internal iliac artery and vein ensheathed by the multiple sheets of the visceral connective tissue of the cardinal ligament. The third layer, the parietal layer, is the external iliac artery and vein on the medial facet of the psoas muscle, and the obturator nerve and the obturator artery and vein, found coursing alongside the anterior side of the obturator internus muscle. The objective of dissections right here is to establish the ureter and the parietal buildings of the third layer. Then, because of the wealthy vascular collateral circulation in the pelvis, the visceral blood vessels within the second layer may be clamped, sutured, and coagulated safely without injuring different pelvic constructions (Video 1. The operator should be aware that these vessels could originate from surrounding parietal vessels but may still be safely clamped, tied, and coagulated. The common iliac artery bifurcates into the interior iliac artery (hypogastric artery) and the external iliac artery, which programs on the medial portion of the anterior floor of the psoas muscle. The exterior iliac vein courses on the medial edge of the psoas muscle, just medial and posterior to the exterior iliac artery. Ureteral harm or occlusion can occur on this area throughout ligation or coagulation of the infundibulopelvic ligament when performing oophorectomy. These similar techniques are essential for sampling and excision of the lymph nodes alongside the common, external, and inside iliac vessels.

Cheap artane 2 mg overnight delivery
When considering laparoscopic surgery, a danger evaluation ought to be performed evaluating the problem degree of the process and potential barriers to success. Two common obstacles encountered in laparoscopic surgery are intra-abdominal adhesions (from earlier surgery, infection, or endometriosis) and the scale of pathology (uterine or adnexal). A concerted effort must be made to anticipate these preoperatively and plan appropriately. A detailed history, physical examination, and, the place acceptable, imaging research, will alert the surgeon to the potential for adhesions or pelvic or stomach masses. Review of earlier operative stories will help put together for the upcoming process as properly. It is somewhat a mirrored image of the entire process of dialogue and counseling throughout which patients are knowledgeable of their analysis, the natural historical past of the disorder, and the complete spectrum of choices for treatment, together with "watchful ready," and forty seven forty eight Principles of laparoscopic surgery Table four. Patient choice Patient preparation Operating room organization Patient positioning Peritoneal entry Creation and imaging of the operative area Tissue and fluid manipulation Cutting and hemostasis Tissue approximation Specimen management and extraction Wound management Postoperative care that may incorporate each medical and surgical management. Similarly, the surgeon ought to present practical expectations for surgical outcomes based on personal experience and acceptable medical literature. Occasionally, unexpected pathology could also be discovered at the time of laparoscopic surgery. Examples embody an unexpected tumor, abnormal appendix, or recognized or suspected pathology extra severe than anticipated. Depending on surgeon talent and availability of sources similar to different consultants, it might be possible to attempt to handle the unexpected discovering at the time of surgical procedure. In some instances, it could be prudent to terminate the process and revisit the plan and method with the patient sooner or later. The bioethical precept of nonmaleficence ("first, do no harm") could also be applied in most of these circumstances. When one can anticipate the presence of concomitant pathology similar to involvement of the appendix in severe endometriosis, appropriate session and consent ought to be obtained. In obese sufferers, working with a multi-disciplinary health-care staff, that might include a dietician and bodily therapist, might facilitate weight loss prior to an elective procedure and attendant discount in associated perioperative dangers. A cautious medical and surgical historical past must be reviewed with the affected person prior to surgery. In such instances, routine laboratory investigations will not be useful but, as an alternative, should be ordered as acceptable based mostly on the medical picture. Expected postoperative restoration together with dialogue of the anticipated time required to be away from work and actions of every day residing. In educational institutions, patients ought to be made aware of the position of trainees corresponding to college students, residents, and fellows of their surgery and perioperative care, in addition to the use of multimedia recording. For instance, surgical administration of endometriosis can differ significantly relying on whether or not the objective is to improve fertility or to scale back pelvic ache. If a specific surgical procedure is deemed outside their scope of follow, applicable referral to surgical specialists should be made. Choice of assistant, nursing, and anesthesiologist can also be necessary to contemplate preoperatively. An assistant for vaginal or uterine manipulation can be often required for complicated gynecologic procedures. Layout of the working room Laparoscopic surgery requires the usage of highly specialized and technical gear; the surgeon is answerable for understanding protected and effective function of those components, including, if necessary, the assembly and troubleshooting of instrumentation. Each surgeon should be aware of acceptable setup of the working room each to optimize workflow and to minimize potential accidents to the affected person and staff. Each surgeon, in addition to the second help (using vaginal manipulator), has a devoted monitor. Scrub nurse and instrument desk place the general dimensions of the working room and areas of "high traffic," because the instrument tables must be positioned to decrease the chance of contamination. Care have to be taken to keep away from placement of equipment in areas that can potentiate the risk of tripping over cables and foot pedals. Surgeon ergonomics Adhering to an appropriate ergonomic place is necessary for the surgeon to reduce strain or musculoskeletal accidents, which usually have a tendency to happen with prolonged and/or tough surgeries. A survey of laparoscopic urology surgeons discovered that 28% and 17% reported frequent neck and shoulder pain, respectively. Common instance of poor surgical posture (shoulder abduction, arrow), which may lead to muscle pressure and injury. Also, observe the usage of instrument holders to facilitate easier transmission when switching instruments.
Green Holy Basil (Holy Basil). Artane.
- What is Holy Basil?
- Diabetes, common cold, influenza ("the flu"), asthma, bronchitis, earache, headache, stomach upset, heart disease, fever, viral hepatitis, malaria, tuberculosis, mercury poisoning, use as an antidote to snake and scorpion bites, or ringworm.
- Are there any interactions with medications?
- Are there safety concerns?
- How does Holy Basil work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97047

Buy generic artane 2 mg on line
Management Any proof of fluid overload ought to lead to quick cessation of the process and possible administration of a diuretic such as furosemide (Lasix). Thus, the cervical canal can be a level of resistance within the effort to acquire entry to the endometrial cavity and, if significant, may be associated with cervical lacerations. Perhaps the most common cause of laceration is the tenaculum positioned on the (usually) anterior aspect of the exocervix for stabilization and countertraction. Factors that enhance the risk of this adverse consequence might embody menopause, nulliparity, cervical stenosis, and the use of giant caliber hysteroscopic methods. Risk-reducing measures Cervical stenosis can increase the risk of trauma related to access. Prostaglandin E1 (misoprostol) or one or more laminaria may be administered 12 to 24 hours prior to a planned hysteroscopic procedure. Misoprostol may be administered vaginally in a dose of 200 or four hundred g orally however may not be as efficacious in postmenopausal women. There is high-quality evidence supporting intraoperative administration of intracervical vasopressin to reduce the force required for cervical dilation by about 50%. Care should be taken to keep away from intravascular injection of vasopressin-containing options. Recognition Careful inspection of the cervix and tenaculum website at the end of the procedure could determine trauma that requires consideration. Management If a cervical laceration happens and is bleeding, it may respond to tamponade using a sponge placed on the finish of a forceps ("sponge stick"). Alternatively, or if such an strategy is unsuccessful, it may be necessary to place a quantity of interrupted 2-0 or 3-0 delayed absorbable sutures for hemostasis. Uterine perforation Adverse events associated to uterine perforation Uterine perforation usually happens due to attempted entry to the endometrial cavity, generally with the passage of a uterine sound, or through the process of cervical dilation. Risk-reducing measures the risk factors for uterine perforation are the same as for cervical trauma together with nulliparity, postmenopausal status, and identified cervical stenosis, generally from earlier surgical procedure, corresponding to conization or loop excision. Preprocedural recognition of these factors permits the clinician to be prepared, and to put together the affected person, for the potential of difficult access. The measures mentioned above to reduce cervical trauma ought to be thought-about, together with using preprocedural laminaria or misoprostol or intraoperative administration of intracervical dilute vasopressin. Using transabdominal ultrasound steering for highrisk sufferers could reduce the risk of uterine perforation. Having the acoustic window afforded by a partially stuffed bladder may be useful, significantly in overweight individuals, or these with a retroverted and/or retroflexed uterus. It is suspected that avoidance of uterine sounds and, the place potential, adopting direct visible entry using the hysteroscope for steering, could scale back the danger of uterine perforation. Recognition Complete uterine perforation is recognized by (1) lack of resistance with passage of the uterine sound or dilator; (2) throughout hysteroscopy, the lack of uterine distension; and/or (3) direct visualization of a transmural defect or extrauterine buildings (Videos 10. Perforation may be suggested by a fast and otherwise unexplained increase in measured fluid deficit. Management If uterine perforation happens with blunt, non-electrosurgical instruments, then the patient could additionally be expectantly managed. If perforation occurs utilizing sharp or activated electromechanical or electrosurgical instruments, at least diagnostic laparoscopy is required to inspect the viscera with subsequent surgical repair as necessary (Video 10. Hemorrhage Causes/mechanisms of hemorrhage the danger of hemorrhage throughout hysteroscopic surgical procedure is generally confined to surgical procedures that transect Complications of hysteroscopic surgery one hundred seventy five vessels within the endometrium or myometrium. Hemorrhage can also occur secondary to perforation with a sharp or activated electrosurgical or electromechanical instrument that transects the periuterine vasculature following uterine perforation. Risk-reducing measures Preoperatively, the influence of intraoperative blood loss can be minimized by correcting anemia, if it exists, with oral or parenteral iron and by taking steps to stop any ongoing heavy menstrual bleeding. Additionally, the usage of intraoperative injections of dilute vasopressin deeply into the cervical stroma has been demonstrated to cut back intraoperative blood loss. Hysteroscopic distension pressure could be elevated as one other technique for tamponade of small-caliber bleeding vessels. For bigger vessels, such increase in stress may simply result in "reversal" of circulate, pushing distension media into the systemic circulation. The patient ought to then be observed for an additional hour prior to discharge if bleeding has subsided. If persistent bleeding is suspected, uterine artery embolization must be thought-about.
2 mg artane otc
Most generally, transmission occurs with comparatively shut contact, usually between related individuals or others dwelling in the identical household. When droplets containing mycobacteria are inhaled and reach the alveoli, a small focus of main infection develops, consisting of the organisms and an inflammatory process mounted by the host. After the preliminary an infection has began, organisms regularly spread by way of lymphatic vessels to draining hilar lymph nodes as well as through the bloodstream to distant organs and different areas of the lung, particularly the apices. This sensitization and development of a cell-mediated immune response usually occur within several weeks of initial exposure. The affected person usually is unaware of the first infection, although a gentle, self-limited febrile sickness could additionally be reported. In a small minority of patients, probably 5% or fewer, defense mechanisms are unable to management the primary an infection, and clinically obvious main tuberculosis outcomes. Even when the first infection apparently has been managed, the tubercle bacillus will not be fully eliminated from the host. A small number of organisms usually stay in a dormant or latent state, not proliferating or causing any apparent energetic disease, however nonetheless potentially viable. However, in some patients, the delicate steadiness between the organism and the host protection mechanisms finally breaks down, sometimes after many years, and a dormant focus of infection Transmission of tuberculosis is by inhalation of small aerosol droplets containing the organism. Such sufferers with lively disease occurring at a time faraway from the first infection are said to have reactivation tuberculosis. For each main and reactivation disease, the lungs are essentially the most commonly affected website. However, with either type of illness, distant organ systems may be concerned because of hematogenous spread during the major part of the infection. In addition, disseminated illness often known as miliary tuberculosis may outcome from the hematogenous spread of the organisms. The danger of developing lively tuberculosis is best throughout the first 2 years after the initial an infection; about one-half of sufferers who develop active disease accomplish that inside this timeframe. Tuberculous illness (or active tuberculosis), on the other hand, is defined by the presence of clinically energetic disease in a number of organ techniques, ideally with affirmation of the prognosis by isolation of M. Other phrases worth defining are people who describe totally different subsets of tuberculous disease. Most frequent are the terms main and reactivation tuberculosis, which refer to disease following the preliminary publicity and illness that reactivates after a period of latency, respectively. Several different terms are sometimes used to describe medical disease on the idea of the presumed pathogenesis. The time period progressive primary tuberculosis reflects primary illness that has not been managed by host defense mechanisms and has continued to be active past the point at which delayed hypersensitivity has developed. As a common rule, cellular immunity develops 2 to 10 weeks after the initial infection, and continuing active disease beyond this time has lots of the options of reactivation tuberculosis. The term postprimary tuberculosis refers to disease beyond the preliminary major infection. Although this time period usually refers to reactivation illness, it generally includes cases of progressive major tuberculosis. The time period reinfection tuberculosis refers to disease in a previously contaminated individual that results not from reactivation of dormant tubercle bacilli but from new publicity to another supply of organisms. It is believed that individuals with prior exposure to tuberculosis who manifest delayed hypersensitivity to the organism are relatively proof against exogenous reinfection from one other supply. The main infection in the lung consists of the organisms and a relatively nonspecific inflammatory response in the concerned region of parenchyma. Regional lymph nodes often turn out to be concerned by native spread of the organism, and the mix of the primary space within the lung (the Ghon lesion) and involved lymph nodes is termed a Ghon complicated. When delayed hypersensitivity is present, both weeks after the primary infection or throughout a period of reactivation illness, a different pathologic pattern emerges. The hallmarks are the presence of (1) granulomas (collections of activated blood- and tissue-derived macrophages termed epithelioid histiocytes surrounded by a rim of lymphocytes), and (2) caseous necrosis (foci of necrosis and softening on the heart of a granuloma).
Purchase discount artane on line
A definition of electrical current, a term often used interchangeably with electrical energy, is the number of electrons transferring past some extent in an electrical circuit throughout a specific amount of time. The fixed polarity circuit is powered by a battery that has constant adverse and optimistic poles that drive electrons to journey in a single course. Increased impedance, subsequently, requires that larger voltage shall be essential to force an equivalent number of electrons through the circuit in a fixed time. Stated in another means, elevated impedance requires larger voltage to keep the same current. The principal setting for most mills is power, the product of current and voltage. When desiccated or carbonized tissue encrusts an active electrode, R will increase and I correspondingly decreases if V remains the identical. Since V is electromotive drive that drives the transit of charged particles throughout a circuit developed by an electrical potential, higher voltage has the propensity to produce higher lateral and deeper thermal necrosis. Accidental contact with family outlet present, which oscillates at 60 Hz, can cause neuronal depolarization leading to ache and tetanic skeletal muscle contraction by depolarization of the neuromuscular junction (Faradic effect). If this depolarization is enough to impact the heart, it can lead to cardiac arrest. The peak of the tower above the bottom and the associated top of the meniscus of the contained fluid create a possible force that can be equated to voltage (V). The impedance is varied by the spigot on the outflow: whether it is opened up (left and center), the "resistance" (R) to circulate is low; if closed down (right), the resistance to circulate is low. The sealed tube contains a water wheel that powers a generator every time the tube is tilted from one aspect to the other. The change in path of the water wheel creates a current that transiently flows in a unique course. These electrosurgical tissue effects result from the conduction of electrons with adequate focus to create variable rates and degrees of tissue heating. Initially, a minimum of, the intracellular temperature heats secondary to the speedy oscillation of ions, together with giant ionized proteins. If the present is targeted and intracellular temperature quickly reaches or exceeds 100�C, a liquid to fuel conversion happens as the intracellular water boils leading to mobile vaporization. Should the present be slightly defocused, and the intracellular temperature exceeds 60�C however is lower than 100�C, the near simultaneous processes of desiccation and coagulation ensue. Desiccation is just lack of intracellular water, while coagulation is heat-induced rupture of hydrogen cross links that then reform with tissue cooling. This signifies that, aside from the patient, the whole circuit is part of the system; grounded circuits require that both the affected person and the generator be related with "ground. In the instance (top), two monopolar instruments are in use: the lively and the dispersive electrode. On the left are bipolar forceps greedy and compressing the blood vessel, the only a half of the patient involved within the circuit. On the proper, the blood vessel is grasped, however the arrows point out that the whole patient is concerned in the circuit. The bigger surface area and substantially lower present density on the dispersive electrode site preclude tissue heating enough to trigger a burn. In different cases, similar to bipolar hysteroscopic needles, the needle electrode is "energetic," while the second electrode is designed to be dispersive and is present solely to full the circuit close to to the goal. The rate of heat production and the intracellular temperature achieved from the conduction of present in residing tissues ultimately determine whether chopping or coagulation of the goal occurs. This fundamentally is determined by the focus of the applied current generally known as current density (Video 3. Practically speaking, manipulating the floor area of the electrode(s) close to to or involved with tissue. On the other hand, a small electrode floor area will, with sufficient current density, lead to mobile and tissue vaporization by the rapid superheating of the intracellular water and the subsequent liquid�gas conversion that we name vaporization. In essence, the extra concentrated the present is, the extra quickly the warmth is produced. Consequently, greater current focus or density is simpler and produces extra heat per unit time. This explains why warmth is concentrated on the energetic electrode and not at the considerably larger dispersive electrode, notably when using monopolar instrumentation.
Best artane 2mg
However, interstitial lung ailments affect all components of the alveolar wall: epithelial cells, endothelial cells, and mobile and noncellular parts of the interstitium. Many authors now prefer the expression diffuse parenchymal lung illness, which is the term usually used on this guide. However, for practical functions the reader should acknowledge that the expressions diffuse parenchymal lung disease and interstitial lung disease typically discuss with the identical group of disorders inflicting inflammation and fibrosis of alveolar structures. Another label, the idiopathic interstitial pneumonias, identifies a group of pathologic entities that symbolize a subcategory of diffuse parenchymal lung disease. This overview is adopted in Chapters 10 and 11 by extra detailed descriptions of specific ailments. A abstract of the pathology of those disorders emphasizes the relative roles of irritation, fibrosis, and granuloma formation, depending upon the actual disorder. The subcategory of idiopathic interstitial pneumonias is described in detail, together with the 6 specific pathologic patterns that comprise this subcategory. Keywords Diffuse parenchymal lung illness Interstitial lung illness Idiopathic interstitial pneumonias Usual interstitial pneumonia Nonspecific interstitial pneumonia Restrictive lung disease Overview of Diffuse Parenchymal Lung Diseases n 133 Table 9. A third class of "mimicking problems" is included in recognition of the truth that a quantity of further well-defined scientific issues can produce diffuse parenchymal abnormalities on chest radiograph. Rather, the reader is urged to first develop an understanding of the pathologic, pathogenetic, pathophysiologic, and scientific features common to these problems. This article is an summary of basic elements of diffuse parenchymal lung illness and refers to particular person diseases solely when essential. Chapter 10 discusses disorders associated with an identifiable etiologic agent; the minority of patients with diffuse parenchymal lung disease are on this class. Chapter 11 discusses diseases for which a selected etiologic agent has not been recognized, representing the vast majority of sufferers with diffuse parenchymal lung illness. These chapters cover only a small variety of the described kinds of diffuse parenchymal disease. The objective throughout is to consider these issues the reader most probably will encounter. The diseases covered in these three chapters are primarily persistent (although sometimes subacute and barely acute) ailments affecting the alveolar structures. Both features incessantly occur simultaneously, although the relative proportions of inflammation and fibrosis differ with the actual cause and period of disease. The basic presumption has been that energetic inflammation is the primary course of and that fibrosis follows as a secondary characteristic. Individual kinds of diffuse parenchymal lung illness may be related to a prominence of a particular inflammatory cell sort, similar to eosinophils in chronic eosinophilic pneumonia. In addition to the presence of inflammatory cells, other attribute pathologic features that help to define a specific dysfunction could also be associated with the alveolitis. These individual patterns are helpful in, and in plenty of instances crucial to , the analysis of a selected pathologic entity. One of the most important and distinctive pathologic options related to several of the diffuse parenchymal lung diseases is the granuloma. These cells are typically accompanied by T lymphocytes throughout the granuloma, often additionally forming a rim around it. When mobile necrosis is current in the center of a granuloma, the entity is termed a caseating granuloma, but diffuse parenchymal lung ailments are associated nearly exclusively with noncaseating granulomas. In distinction, Diffuse parenchymal (interstitial) lung illnesses are characterized pathologically by variable amounts of inflammation and fibrosis. Photomicrograph of diffuse parenchymal lung illness reveals markedly thickened alveolar partitions. Low-power photomicrograph of transbronchial lung biopsy pattern from affected person with sarcoidosis. Numerous confluent granulomas throughout whole specimen obliterate regular pulmonary architecture.

Trusted 2 mg artane
It is synthesized regionally to a big extent, though a fraction additionally originates from serum IgG. It has numerous organic properties, corresponding to agglutinating particles, neutralizing viruses and bacterial toxins, serving as an opsonin for macrophage phagocytosis of bacteria, activating complement, and inflicting lysis of gram-negative micro organism in the presence of complement. The total position of the humoral immune system in respiratory defenses includes protecting the lung in opposition to quite lots of bacterial and, to some extent, viral infections. The clinical implications of this function and the consequences of impairment within the humoral immune system are discussed within the section on defects in the adaptive immune system. Major components of the adaptive immune system operative in the respiratory tract are: 1. IgG 292 n Principles of Pulmonary Medicine Cellular Immune Mechanisms Cellular immune mechanisms, these mediated by thymus-dependent (T) lymphocytes, also function as a part of the overall protection system of the lungs. Sensitized T lymphocytes produce quite a lot of soluble, biologically energetic mediators referred to as cytokines, a few of which. T lymphocytes are also able to interacting with the humoral immune system and modifying antibody manufacturing. Two essential kinds of T lymphocytes have been nicely characterised on the premise of particular cell floor markers and practical characteristics. One essential function for the mobile immune system is to shield in opposition to bacteria that have a sample of intracellular development, especially M. In addition, the cellular immune system has a important role in the dealing with of many viruses, fungi, and protozoa. Although separating the immune protection of the lung into different categories is necessary for discussion functions, all of those limbs are deeply intertwined, and dysfunction in a single facet will probably trigger problems in different elements of the system. Development of a respiratory an infection typically signifies that a variety of protection mechanisms have been overcome by the infecting organism. As a end result, respiratory infections may ensue, and the analysis of the precise forms of infections associated with each kind of defect is clinically helpful. Impairment of Physical Clearance the best impairment of physical clearance to understand is the shortcoming to cough effectively. Three factors are required to generate the high velocities of an efficient cough: (1) a large inspiration, (2) a rise in intrathoracic stress in opposition to a closed glottis, and (3) a coordinated expiratory blast throughout which the glottis opens. Considering each of these steps, it turns into simpler to appreciate why sure sufferers have problem with clearing inhaled particles and respiratory secretions. All these sufferers are prone to respiratory tract infections, even if the underlying immune methods are regular. Other physical or anatomic components that influence deposition and clearance of particles embody genetic abnormalities and environmental elements affecting the mucociliary transport system. Especially fascinating information has been provided by a genetic abnormality termed primary ciliary dyskinesia, also sometimes known as both the dyskinetic cilia syndrome or the immotile cilia syndrome. In this dysfunction, a defect in ciliary construction and performance results in absent or impaired ciliary motility and therefore to ineffective Lung Defense Mechanisms n 293 mucociliary clearance. More than 20 kinds of defects are acknowledged, however the most common is the absence of dynein arms on the microtubules. Clinically, the impairment in mucociliary clearance is associated with continual sinusitis, chronic bronchitis, and bronchiectasis. In males, the sperm tail, which has a structure much like that of cilia, is abnormal, leading to poor sperm motility and infertility. The dysfunction known as Kartagener syndrome, which consists of the triad of persistent sinusitis, bronchiectasis, and situs inversus, is a variant of main ciliary dyskinesia (see Chapter 7). Normal ciliary motion in a specific direction is believed to be liable for the normal rotation of the center and positioning of intraabdominal organs throughout embryogenesis. When ciliary function is significantly disturbed, positioning of the heart and intraabdominal organs turns into random, thus accounting for the situs inversus present in approximately 50% of patients with main ciliary dyskinesia. Viral respiratory tract infections frequently trigger short-term structural harm to the tracheobronchial mucosa. Functionally, alteration of the mucosa is related to impaired mucociliary clearance, which can retard the transport of invading micro organism out of the tracheobronchial tree. This is doubtless one of the mechanisms by which viral respiratory tract infections predispose the person to complicating bacterial superinfections. Exposure to cigarette smoke is crucial clinically and possibly contributes to the predisposition of heavy people who smoke to recurrent respiratory tract infections. High concentrations of O2, such as 90% to 100 percent inhaled for more than a number of hours, seem to be associated with impaired mucociliary operate.
Real Experiences: Customer Reviews on Artane
Armon, 48 years: Consequently, activation of the sympathetic nervous system favors bladder storage.
Bozep, 49 years: The pericardium, pleura, kidney, peritoneum, adrenal glands, bones, and central nervous system every could also be involved, with symptoms ensuing from the particular organ or area affected.
Merdarion, 37 years: After exposure to an initiating stimulus occurs, a complex sequence of interrelated events is responsible for propagation of the illness.
Yasmin, 59 years: Peritoneal dissemination complicating morcellation of uterine mesenchymal neoplasms.
8 of 10 - Review by V. Lukjan
Votes: 56 votes
Total customer reviews: 56
References
- Seppalainen AM, Tola S, Hernberg S, Kock B. Subclinical neuropathy at 'safe' levels of lead exposure. Arch Environ Health. 1975;30:180-183.
- Harrison-Phipps KM, Nichols FC, Schleck CD, et al. Solitary fibrous tumors of the pleura: results of surgical treatment and long-term prognosis. J Thorac Cardiovasc Surg 2009;138(1): 19-25.
- Melo KFS, Mendonca BB, Billerbeck AEC, et al: Clinical, hormonal, behavioral, and genetic characteristics of androgen insensitivity syndrome in a Brazilian cohort: five novel mutations in the androgen receptor gene, J Clin Endocrin Metab 88:3241n3250, 2003.
- Berna MJ, Annibale B, Marignani M, et al. A prospective study of gastric carcinoids and enterochromaffin-like cell changes in multiple endocrine neoplasia type 1 and Zollinger-Ellison syndrome: identification of risk factors. J Clin Endocrinol Metab 2008;93:1582.