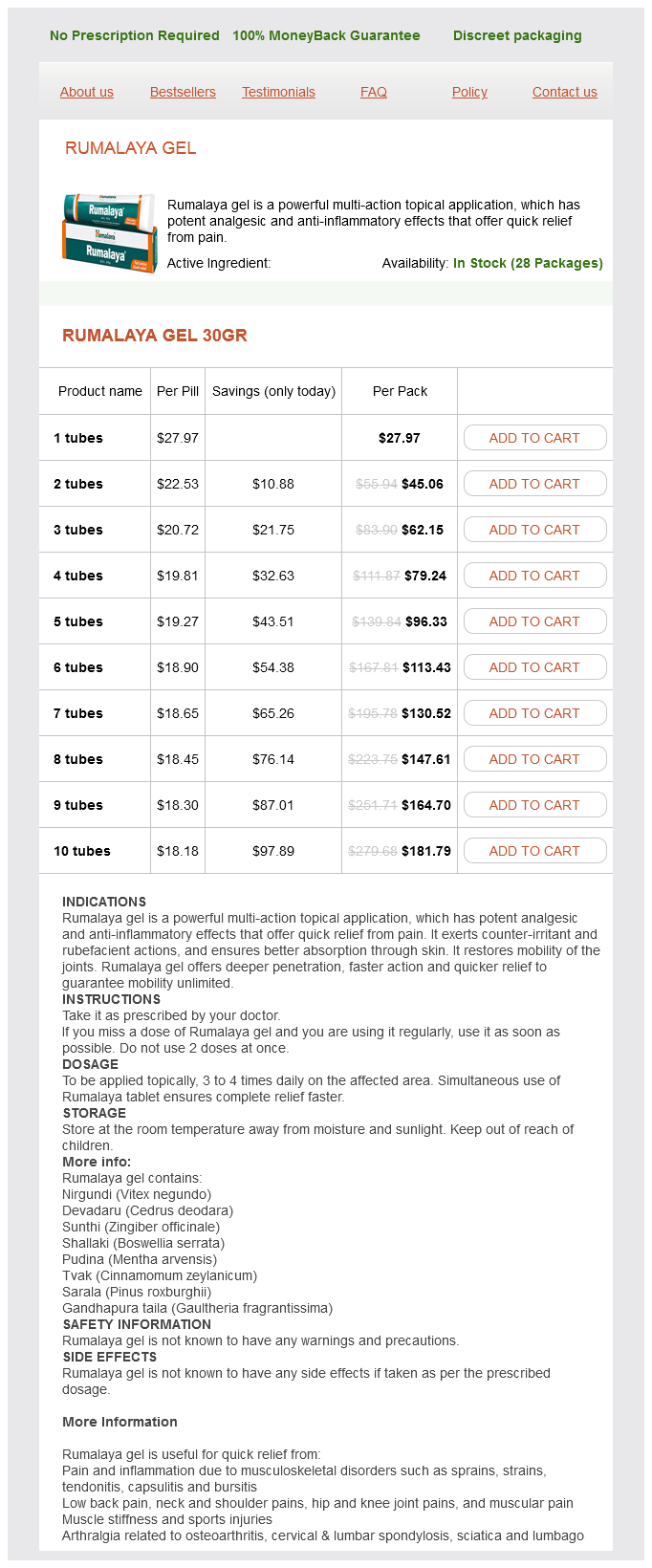
Rumalaya gel dosages: 30 gr
Rumalaya gel packs: 1 tubes, 2 tubes, 3 tubes, 4 tubes, 5 tubes, 6 tubes, 7 tubes, 8 tubes, 9 tubes, 10 tubes

Cheap rumalaya gel 30gr mastercard
Filum ependymomas and cauda equina nerve sheath tumors happen with about equal frequency. Myxopapillary ependymomas are by far the most typical histological kind encountered within the filum terminale. Their histological look consists of a papillary association of cuboidal or columnar tumor cells surrounding a vascularized core of hyalinized and poorly mobile connective tissue. Meningiomas Meningiomas are the second most typical intradural extramedullary spinal tumor after schwannomas. The feminine preponderance seen in intracranial meningiomas is even more pronounced in the spine, with surgical sequence reporting female/male ratios of 4:a hundred and ten to as excessive as 9:1. This formulation likely influences the finding that the majority of spinal meningiomas are intradural, ex- Paragangliomas Paragangliomas are uncommon tumors that originate from the neural crest and may arise from the filum terminale or cauda equina. Identification of dense core neurosecretory granules on electron microscopy establishes the analysis. Complete resection is usually potential except for large tumors which are tightly adherent to the cauda equina. Diagnostic Imaging Magnetic resonance imaging is the procedure of selection for the analysis and analysis of intradural tumors. The tumor occupies almost the whole cross-sectional space of the spinal canal on the axial image. Note the proximity and displacement of the distal conus medullaris along with the distinguished draining veins on the spinal twine floor. The measurement of the tumor precluded secure en-bloc resection, so a subtotal piecemeal resection was accomplished. Surgical resection of these tumors will accomplish either objective in the overwhelming majority of patients. Surgery is clearly indicated in patients with symptomatic tumors, notably those with massive tumors producing vital compression of the spinal twine or cauda equina. For patients with smaller tumors or these with minimal subjective symptoms, it could be affordable to comply with them each clinically and radiographically over time. For small and asymptomatic tumors, interval radiographic surveillance may also be beneficial. An exception for observation of asymptomatic tumors is the midline filum/cauda equina tumor. There are several issues that must be considered within the planning of surgical resection of these tumors. The dimension, location (both in the axial and sagittal planes), spinal stage, relationship of the tumor to the spinal twine, as nicely as tumor vascularity and consistency are relevant in this regard. The overwhelming majority of intradural extramedullary tumors may be safely accessed and eliminated via a normal posterior laminectomy. Even most ventrally positioned tumors can be accessed posteriorly as a end result of lateral spinal cord displacement or rotation enables a safe hall to debulk and take away most ventrally situated tumors. Instrumented fusion that extends one degree above and under the facetectomy is normally carried out. Ventral meningiomas that encase the vertebral artery and lower cranial nerves at the foramen magnum�upper cervical area or massive dumbbell extension into the upper cervical region could preclude protected surgical resection. Multifractionated radiation remedy is considered for patients following subtotal resection of myxopapillary ependymomas of the filum terminale. Benign spinal nerve sheath tumors: their prevalence sporadically and in neurofibromatosis varieties 1 and 2. Longterm outcome after removal of spinal schwannoma: a clinicopathological examine of 187 instances. They might present as incidental findings on imaging research or present with profound neurologic deficits. Symptoms range greatly and could also be as refined as mild ache or as drastic as scoliosis with important neurologic deficits. As with bone tumors in other areas, night time pain is incessantly related to neoplasm. Primary benign tumors usually occur within the youthful population with a barely greater prevalence in males.
Generic rumalaya gel 30gr visa
Muscle retraction to obtain the lateral to medial pedicle trajectories and subsequent displacement of adjacent segments might cause errors in registration. To cut back error, think about cannulating the pedicle with a drill with out downward and inward strain to reduce the deformation of the spine in relation to the reference array. Navigate/instrument cervical pedicle screws first, with the reference frame near the cervical backbone. Move the reference array one or two ranges caudal to the last thoracic/ lumbar instrumented degree. Then obtain an O-Arm scan of the thoracic and lumbar levels and navigate or instrument the thoracic or lumbar screws. Cervical pedicle screw fixation in 100 circumstances of unstable cervical injuries: pedicle axis views obtained utilizing fluoroscopy. J Neurosurg Spine 2006;5:488�493 Yoshimoto H, Sato S, Hyakumachi T, Yanagibashi Y, Masuda T. Indirect posterior reduction and fusion of the traumatic herniated disc through the use of a cervical pedicle screw system. Placement of pedicle screws within the human cadaveric cervical backbone: comparative accuracy of three techniques. Cervical pedicle screws: standard versus computer-assisted placement of cannulated screws. Intraoperative, full-rotation, three-dimensional image (O-arm)-based navigation system for cervical pedicle screw insertion. Intra-operative computer navigation guided cervical pedicle screw insertion in thirty-three complicated cervical backbone deformities. J Craniovertebr Junction Spine 2010;1:38�43 Ishikawa Y, Kanemura T, Yoshida G, Ito Z, Muramoto A, Ohno S. Clinical accuracy of three-dimensional fluoroscopy-based computer-assisted cervical pedicle screw placement: a retrospective comparative study of typical versus computer-assisted cervical pedicle screw placement. J Neurosurg Spine 2010;13:606�611 Ito Y, Sugimoto Y, Tomioka M, Hasegawa Y, Nakago K, Yagata Y. J Neurosurg Spine 2008;9:450�453 Abumi K, Shono Y, Ito M, Taneichi H, Kotani Y, Kaneda K. Cervical pedicle screw placement using the "key slot method": the feasibility and learning curve. Assessment of pedicle perforation by the cervical pedicle screw placement using plain radiographs: a comparison with computed tomography. Spine 2012;37:280�285 Onishi E, Sekimoto Y, Fukumitsu R, Yamagata S, Matsushita M. Reconstruction of the subaxial cervical backbone utilizing pedicle screw instrumentation. One-stage posterior decompression and reconstruction of the cervical backbone by using pedicle screw fixation systems. Indications and Contraindications the indications embody fixed sagittal malalignment of the cervical spine (mid- to low subaxial cervical spine) affecting horizontal gaze, persistent ache associated to cervical sagittal imbalance regardless of conservative treatment, and excessive pelvic tilt causing low again pain driven by the cervical deformity following the failure of conservative management. This process is contraindicated within the presence of serious osteoporosis or debilitating comorbidities. Potential disadvantages are that this process may be very complex, and it requires significant expertise. Furthermore, this process ends in a big osteotomy and elevated blood loss in contrast with other cervical osteotomies. Choice of Operative Approach the posterior approach is the appropriate one for this technique. Preoperative Testing the deformity should be evaluated by anterior/posterior and lateral cervical radiographs along with dynamic lateral flexion/ extension views. If important ventral compressive pathology (disk, osteophyte) is current, a ventral decompressive process may first be carried out earlier than the correction of the deformity. This determination contributes to the protection of the process, because if the vertebral artery entered at C7, the procedure becomes exceedingly more complex and will should be aborted in some cases. Sequential lumbar or custom wedge-shaped spinal taps are used to decancellate the C7 vertebral body mixed with osteotomes and down-pushing curettes to create as extensive a wedge as potential. A 30-degree angle may be chosen primarily based on standard techniques used in the thoracolumbar backbone and as a place to begin intraoperatively.
Purchase rumalaya gel 30 gr fast delivery
Following cervical lateral mass screw fixation, the fusion fee is excessive and carries a low threat of complications. Safe placement of lateral mass screws requires familiarity with the cervical anatomy. Multiple techniques have been described with completely different screw entry factors and trajectory angles to stop neurovascular harm. Choice of Operative Approach Roy-Camille et al3 initially described the screw entry in the midpoint of the lateral mass with a 10-degree lateral trajectory. Magerl et al4 described the screw entry 2 mm medial and caudal to the midpoint of the lateral mass with a 25-degree lateral and 40to 60-degree cranial (parallel to facet joint) trajectory. When comparing both techniques, the cephalad projection offered by the Magerl method decreased the dangers of violating the aspect joint. This chapter discusses the Magerl technique, specializing in C3�C6 lateral mass fixation. Indications � � � � Cervical instability as a outcome of trauma Reconstruction for degenerative and inflammatory illnesses or neoplasms Cervical deformity or malformations Prevention of postlaminectomy kyphosis Contraindications � � Metabolic bone illness Fracture or previous deformity of the lateral mass Surgical Procedure Positioning In sufferers with cervical myelopathy, extra care ought to be taken to avoid neck motion throughout intubation. Ideally, fiberoptic intubation should be carried out and the affected person should be evaluated for any adjustments in neurologic standing which will have occurred Objective � Obtain spinal stability by fixation and fusion while maintaining or bettering neurologic operate associated with the spinal pathology. General anesthesia applicable for electrophysiological monitoring is used, and the affected person is rigorously placed within the prone position on chest rolls. A lateral fluoroscopy or X-ray could additionally be utilized to ensure proper cervical spinal alignment and to assist localize the pathology. The shoulders are taped down and the legs are flexed on the knees to enable maximal radiological visualization of the cervical spine. Bony prominences are padded, after which the patient is sterilely prepped in the standard fashion. Bleeding from the venous plexus lateral to the lateral plenty may happen and may be coagulated with electrocautery or an absorbable gelatin sponge. Great care should be taken to not disrupt the side joints above and below the concerned ranges of fixation/stabilization to avoid late instability or fusion at those ranges. The capsular ligaments and gentle tissue from the concerned facet could be removed with a small pituitary rongeur and by sweeping from medial to lateral with a curette. Reduction If discount is required and closed discount was not profitable, open discount may be performed at this point. A curette or comparable instrument could additionally be wedged into the side joint to facilitate discount. If unsuccessful, a high-speed drill can be used to remove part of the superior articular means of the inferior vertebrae to facilitate realignment to the normal anatomic state. An electrocautery dissection is used to totally expose the aspect joints and lateral borders of the lateral lots in a subperiosteal fashion. Dissecting more lateral than the lateral border of the lateral 38 Subaxial Cervical Lateral Mass Screw Fixation 245 Instrumentation the middle of the lateral mass may be situated by defining the border between the lamina and the lateral mass. In many circumstances, a small up-going curette can be utilized to outline the lamina�facet junction. The lateral mass can then be cut up into 4 quadrants, and the entry point is identified and marked. A high-speed drill or axe is used to pierce the outer cortex of the bone at the entry level. This reduces the risk of the drill slipping over the lateral mass with screw placement, and supplies entry through the superficial cortical bone. After confirming that the joint capsule and gentle tissue are removed from the involved facets, the joints may be decorticated with a high-speed drill with a small drill bit. In our clinical follow, we use a high-speed drill to partially drill into the superficial aspect. This defines the borders of the lateral mass and likewise decorticates the side margins for inter-facet fusion. Using a 4-0 Penfield, arthrodesis merchandise can be positioned into the superficial portion of the aspect. The trajectory of the screws is 30 levels laterally and 40 to 60 levels cephalad (parallel to the facets) to keep away from neurovascular injuries and unintended fixation of the superior aspect of the following vertebra inferiorly.
Buy 30 gr rumalaya gel otc
We have utilized screw-and-rod constructs in addition to customized contoured threaded titanium loops for occipitocervical fixation with autologous rib graft for the osseous assemble. A number of cranium base approaches have expanded from the essential anterior, lateral, and posterior routes to the foramen magnum. Irreducible dorsal or lateral encroachment is approached dorsally or laterally, respectively. In either circumstance, if instability is current, posterior instrumentation with fixation and fusion is commonly needed. Basilar impression (platybasia): a weird developmental anomaly of the occipital bone and higher cervical spine with striking and deceptive neurologic manifestations. Craniovertebral junction database evaluation: incidence, classification, presentation, and therapy algorithms. Primary craniovertebral anomalies and the hindbrain herniation syndrome (Chiari I): knowledge base analysis. All 19 sufferers have been both untreated or managed conservatively in a cervical collar. These studies and others strongly suggest that, as quickly as cervical myelopathy is established in patients with rheumatoid cervical spine illness, the pure history with out surgical intervention is grave, and mortality is extra frequent than beforehand believed. Additionally, the incidence of cervical myelopathy and therefore mortality from myelopathy is probably going underestimated in rheumatoid patients. Progressive pain, immobility, and weak spot are often attributed to exacerbation of the systemic illness course of somewhat than to neural compression. A historical past of corticosteroid use, seropositivity for rheumatoid issue, the finding of rheumatoid subcutaneous nodules, and the presence of mutilating peripheral articular disease are all predictive of larger development of cervical instability and neurologic injury. In a metaanalysis of 1,749 sufferers within the published literature, Casey and Crockard4 found that 32% (range, 5. Over half of these affected in this analysis (17%) had neurologic signs or signs. Joints that finally develop severe destruction normally become symptomatic within the first year of illness onset. Additional neurologic involvement not referable to the cervical spine includes compression neuropathies similar to carpal tunnel syndrome, diffuse sensorimotor neuropathies, and mononeuritis multiplex. These modifications are as a result of the same host of inflammatory cells and mediators that causes destruction of the joints within the appendicular skeleton. Although the inciting reason for irritation is unclear, the inflammatory process itself is nicely described. Lymphokines, secreted by mononuclear cells, stimulate antibody production and the discharge of extra degradative products. The influx of mixed fluid and inflammatory mediators produces the pain, swelling, and erythema that characterize rheumatoid synovitis. Granulation tissue known as rheumatoid pannus then forms in the affected joint on account of proliferating fibroblasts and inflammatory cells. The pannus produces collagenase and different proteolytic enzymes, resulting in injury to adjacent cartilage, tendons, and bone. The ensuing destruction leads to cartilage loss, bony erosions, cranial settling, tendon ruptures, and ligamentous laxity. Subsequent neurologic injury secondary to compression of the spinal cord, nerve roots, or vertebral arteries can result from direct impingement by the proliferating synovitic pannus or from repetitive bony compression as a end result of vertebral subluxation and instability. As against osteoarthritis, in the rheumatoid course of, lesions from the joints of Luschka lengthen into the disk areas and vertebral bodies with out osteophytosis. Cranial Settling Cranial settling is one other type of basilar impression (acquired basilar invagination or secondary basilar invagination), which results from erosion of bone and compression of the lateral mass of the atlas vertebrae with subsequent rostral migration of the axis vertebrae that can outcome in compression of the ventral cervicomedullary junction by the odontoid course of. The occipital condyles may completely erode by way of the lateral plenty of the atlas, separating them into anterior and posterior pieces. The anterior component might migrate caudally over the axis body, whereas the posterior element often shifts upward. Cranial settling, most incessantly presents with occipital or suboccipital pain, usually with radiation towards the vertex. Limb paresthesias, vertigo, diplopia, and transient blackout spells were complaints in 55% of sufferers with cranial settling. Abnormal neurologic indicators similar to hyperreflexia and Babinski responses were presents in 80% of patients.
Diseases
- Trevor disease
- Magnesium defect in renal tubular transport of
- BANF acoustic neurinoma
- Necrotizing encephalopathy, infantile subacute
- Central core disease
- Mirhosseini Holmes Walton syndrome
- Cataract, congenital ichthyosis
- Methylmalonic aciduria microcephaly cataract
- Renal hypertension
- Adrenal cancer
Buy 30 gr rumalaya gel
Next, the muscular attachments to C2 and C3 are launched from medial to lateral until the aspects are outlined. The self-retaining retractors are inserted deeper to preserve the exposure for the next. Conclusion Posterior publicity of C1-C2 needs to be carried out for a myriad of pathologies affecting the atlantoaxial area. This is most important when addressing the atlantoaxial segment, which is encased with a dense venous network. Postoperative Care the postoperative care is decided by the exact operative approach performed and is discussed in Chapters 16 and 18 to 20 in this textbook. Potential Complications and Precautions Excessive neck flexion and extension ought to be avoided whereas positioning the patient. The vertebral artery is at risk of injury during exposure, and the dissection should be limited to 1. Ponticulus posticus on the posterior arch of atlas, prevalence evaluation in symptomatic and asymptomatic sufferers of Gulbarga inhabitants. Traynelis Atlantoaxial instability may be induced by traumatic, congenital, neoplastic, infectious, rheumatologic, degenerative, and iatrogenic etiologies. The frequent results of every of those entities is a narrowed spinal canal that may produce intermittent or persistent impingement of the neural components or structural changes inflicting neurologic deterioration, deformity, or ache. The first step in performing any atlantoaxial fusion surgical procedure involves enough exposure of C1 and C2 to enable performing the technique to be used, adopted by placement of the instrumentation and fusion substrate. Most surgeons use one of three common posterior stabilization choices: sublaminar wiring, laminar clamps, and screw fixation. One of the earliest reviews of posterior cervical wiring of the lamina of C1 and C2 was by Mixter and Osgood,eight who in 1910 treated an odontoid fracture in a 15-year-old boy utilizing a braided silk loop passed beneath the C1 arch and across the C2 spinous process. Gallie9 subsequently described in 1939 his technique of posterior atlantoaxial wiring, which was supplemented with an H-shaped bone graft to aid in arthrodesis. It was not till virtually 40 years later that Brooks and Jenkins10 offered an alternative method of posterior C1-C2 laminar wiring. Dickman and Sonntag et al11 reported their further modification of the posterior wiring approach in 1991. Posterior atlantoaxial wiring biomechanically acts primarily as a tension band, and as such offers outstanding resistance to flexion. Placement of a graft between the dorsal elements of C1 and C2 serves to restrict extension whereas axial rotation is resisted principally by friction between the cable and posterior components. Postoperative bracing is necessary (rigid orthosis or optimally a halo vest) to optimize the fusion price. Although relatively inexpensive and straightforward to perform, posterior wiring currently is most often employed as an adjunct to screw-based fixation strategies of the atlantoaxial section to enhance the stiffness of the assemble. The anterior tubercle serves as an attachment site for the longus colli muscle, and posteriorly the fovea dentis serves because the articulation point for the odontoid means of the second cervical vertebra (C2). The posterior arch supplies a easy edge for the attachment of the posterior atlanto-occipital membrane. The sulcus arteriae vertebralis is current behind every superior articular process and represents the superior vertebral notch. The undersurface of the posterior arch supplies an attachment floor for the posterior atlantoaxial ligament. The second cervical vertebra (C2) or axis forms a pivot around which the first vertebra rotates. It artic- ulates with the inferior side surface of C1 to permit rotation of the top. Anteriorly, at the stage of the superior aspect, the essential transverse atlantal ligament (a component of the cruciate ligament) traverses the C1 ring, dividing the vertebral foramen into an anterior half, which encases the dens, and a posterior part, which incorporates the spinal wire. Therefore, there are three atlantoaxial joints: two lateral mass articulations and the atlantodental joint. In some cases, the sulcus for the vertebral artery on the dorsal side of the atlas could additionally be utterly coated by an anomalous ossification, termed the ponticulus posticus. The presence of an unidentified ponticulus posticus might result in iatrogenic damage to the vertebral artery.
Buy cheap rumalaya gel 30 gr line
This muscular rim is denervated and have to be tagged each three cm for later reattachment. Using a different-color suture for all sides of the diaphragm can help subsequent closure. The majority of the diaphragm remains innervated and totally practical as a outcome of the phrenic nerve inserts centrally and radiates peripherally. The undersurface of the diaphragm is bluntly dissected from the retroperitoneum again to the crus. The pleura is then recognized, incised, and dissected anteriorly, elevating it from the spine with the diaphragm. The crus of the diaphragm can additionally be incised, leaving a small cuff on the backbone for later approximation. The lung is deflated and packed, and a rib spreader is launched to maximize the exposure. The vascular community of segmental vessels lies anterior to the vertebral bodies and these vessels are mobilized and ligated. Two ligatures should be applied on the aortic stump, and ligation have to be 1 cm from the vertebral foramen to avoid disruption of the anastomotic blood supply. Care must be taken in the course of the ligation process to keep away from damage to the posterior sympathetic chain. To facilitate visualization of the spine, the proximal attachment of the psoas muscle could also be incised and dissected posteriorly with a sharp elevator. At this level, the vertebrae are visualized and can be dissected to the neural foramina, pedicle, and anterior longitudinal ligament. Once the surgeon has oriented the surgical working space throughout the anatomy, the diskectomy, decompression, and instrumentation can proceed. If indicated, the vertebral body could be removed after excision of the intervertebral disks above and below the operative stage. For acute fractures, the vertebrectomy can be carried out with a mixture of rongeurs and curettes. After adequate decompression is achieved, strut grafting is required for reconstruction, and stabilization is achieved with an applicable plating system. Closure Closure is initiated by approximating the diaphragmatic crus with nonabsorbable suture. A chest tube is placed by way of a separate stab incision beneath direct visualization by way of the thoracic portion of the exposure to evacuate blood and air. Two tubes could additionally be necessary-one aimed superiorly to evacuate air and one aimed inferiorly to evacuate blood. The periosteum and intercostal muscle layers are closed in airtight trend with running suture. The transversalis fascia and aponeurosis of the transverses abdominus and oblique muscular tissues are repaired to stop hernia formation. Complications the complication profile for the thoracoabdominal strategy contains potential respiratory, vascular, and stomach damage. Complications involving the stomach might embody injury to the stomach, colon, kidney, ureter, or spleen. Peritonitis might end result from unrecognized intraperitoneal injury and should be suspected if prolonged ileus and abdominal pain are present. All problems of thoracic surgical procedure might happen, including atelectasis, pneumonia, pleural effusion, pulmonary edema, and coronary heart failure. Hemorrhage, delayed or quick, is feasible and should trigger spinal cord compression if current within the epidural house. Finally, harm of the artery of Adamkiewicz with resultant spinal twine infarction is possible if intersegmental arteries are ligated too close to the neural foramen. Postoperative Care Postoperative care is fairly routine in sufferers undergoing the usual open thoracoabdominal strategy. A bowel routine is beneficial, significantly for sufferers requiring a major quantity of narcotic medicines. Daily chest radiographs enable the surgeon to monitor for pneumothorax and pleural effusions.
Discount 30gr rumalaya gel fast delivery
Division of a number of of the dentate ligament attachments to the lateral dura might enhance access to ventral tumor extension. A well-defined arachnoid plane typically exists between the spinal twine and tumor capsule. Depending on the dimensions and consistency of the tumor, inside debulking with an ultrasonic aspirator or laser facilitates visualization and growth of the tumor margins. Cauterization of the dural base could scale back bleeding from extremely vascular or friable lesions. For extra lateral and ventral tumors, cauterization of the tumor origin is preferred because of the difficulty of dural reconstruction in these areas. Filum Terminale Tumors the basic ideas of intradural surgical exposure additionally apply to filum terminale tumors. The filum terminale is cauterized above and below the tumor and divided, and the tumor is fastidiously rotated out of the canal. It is usually not possible to obtain en-bloc resec- 72 Intradural Extramedullary Tumor Resection 465 a b c. The filum is differentiated from the encompassing cauda equina nerve roots by its white shade and vascularity. For example, the tumor may lack sufficient internal integrity and fall apart with even light manipulation. The tumor may be too large to tease out with out placing unacceptable quantities of traction on overlying nerve roots. Functional roots could appear to course instantly via the substance of the tumor. Safe resection could be impossible in these circumstances as a outcome of the dearth of supportive connective tissue matrix. Potential Complications and Precautions Most issues relate to the wound and thromboembolic occasions. Delayed pseudomeningoceles without skin drainage may be adopted conservatively for many weeks in sufferers with no significant signs because they usually spontaneously resolve. A small dural defect can normally be recognized as the cause for the persistent leak and may be primarily repaired with suture and a small muscle graft. Postoperative Care If a watertight dural closure is achieved, a subarachnoid lumbar spinal drain is unnecessary. The patient is kept flat in mattress for forty eight with sequential compression units and a Foley catheter. Timely diagnosis and early treatment in symptomatic patients utilizing up to date neurosurgical strategies result in favorable clinical outcomes for many sufferers. Spinal meningiomas in sufferers youthful than 50 years of age: a 21-year expertise. Midline ventral intradural schwannoma of the cervical spinal wire resected via anterior corpectomy with reconstruction: technical case report and review of the literature. Minimally invasive removing of thoracic and lumbar spinal tumors utilizing a nonexpandable tubular retractor. McCormick Surgery represents the best treatment of benign wellcircumscribed tumors, which represent the majority of intramedullary neoplasms. Patient Selection the predominant good factor about surgery for an intramedullary tumor is prophylactic. Preservation, rather than restoration, of neurologic function is the most likely consequence after profitable surgical therapy. In reality, important improvement of a severe or long-standing preoperative neurologic deficit not often occurs after a technically profitable surgical excision. Surgical morbidity is also greater in sufferers with more vital preoperative deficits. This creates a therapeutic irony in which the danger of surgical procedure is definitely decrease in patients with minimal or no objective neurologic deficit. Thus, early clinical diagnosis and, if potential, definitive preliminary remedy are critical to profitable clinical administration of most intramedullary tumors. A therapeutic dilemma arises, however, in the asymptomatic patient in whom an incidental intramedullary spinal wire lesion has been discovered. A posterior column deficit is a typical consequence of a dorsal median myelotomy; thus, some extent of morbidity usually accompanies even essentially the most successful surgical elimination. In fully asymptomatic sufferers, subsequently, statement with serial scientific and radiological follow-up is an appropriate administration strategy for most sufferers, particularly these with situations similar to neurofibromatosis or von Hippel�Lindau disease.
Rumalaya gel 30 gr sale
This area is then fastidiously developed additional, and the sacral promontory, left ureter, and iliac vessels are recognized. Direct pressure on the left ureter is averted by putting the retractor superficial to it, so that the ureter can be visualized through the process on the right aspect of the field (anterior to the spine and attached to the peritoneum). The position and integrity of the most important vessels, ureter, and backbone are identified and verified. The vasculature is then fastidiously dissected, employing sharp approach for arteries and blunt dissection to the comparatively thin-walled veins. A gel-filled roll or foam axillary roll may be placed beneath the lumbosacral junction to generate a lordotic position if wanted. A midline incision is produced from just distal to about two thirds of the way to the pubic symphysis umbilicus. A dissection aircraft is then carried simply deep to the left rectus muscle, permitting the endoabdominal fascia and peritoneum to fall away from the posterior rectus muscle. The endoabdominal fascia is then incised vertically utilizing tissue scissors, and blunt dissection is used to sweep the peritoneum. Once the L5-S1 disk is correctly uncovered and recognized, a generous annulotomy is sharply performed, releasing enough disk on the anterolateral corners to prepare for lordotic distraction. A Cobb elevator and numerous curettes can then be used to take away further disk material and separate the cartilaginous finish plates from the vertebral bodies. It is important to take away and launch enough disk to generate most mobilization for deformity correction and concurrently achieve enough arthrodesis of both end plates for fusion. Furthermore, nice care must be taken to preserve the subchondral osseous structure of the end plates to forestall early graft subsidence. Screws are then introduced by way of the interbody system via manufactured screw holes to secure the cages and stop dislodgment. Hemostasis is obtained through cautious bipolar cautery and packing with topical hemostatic agents in the deeper spaces. The retractors are carefully eliminated, with thorough inspection to guarantee enough hemostasis. The peritoneum is gently swept again in place and inspected for rents, that are closed primarily with Vicryl suture. The belly fascia is then closed meticulously to stop hernia formation, and the remainder of the wound is closed in anatomic layers. The vessels are then carefully mobilized circumferentially, with small branches being rigorously identified, ligated, and divided. The center sacral vessels over the L5-S1 disk are recognized, encircled with an angled clamp, and double clipped earlier than being divided. There is typically one middle sacral artery with two veins, one of which branches off the left common iliac vein and programs towards the left border of the lumbar spine. This vessel is commonly missed and might trigger important blood loss if it is avulsed. The unfastened areolar tissue over Postoperative Care Postoperative care after anterior approaches is centered mainly on careful food plan advancement and prevention of venous thromboembolism. Potential Complications and Precautions the most typical complications throughout anterior approaches to the lumbar spine are venous accidents. Circumferential exposure, management, and restore of the massive venous constructions could be exceedingly tough as a outcome of their thin partitions and the deep operative site with complex anatomy. Most small venous tears may be repaired with surgical clips deployed tangentially to the vein. Risk factors for vascular thrombosis (such as atherosclerosis, fibromuscular dysplasia, or venous thromboembolism) must be identified preoperatively. When working on a affected person with atherosclerotic iliac vessels, you will want to frequently examine a distal left iliac pulse all through the operation. A pulse oximeter can also be used on both lower extremities to monitor differential oxygen saturations. If a typical iliac artery thrombosis occurs, 5,000 models of intravenous heparin is given instantly while circumferential proximal and distal management of the vessel is rapidly obtained and an open thrombectomy is then performed. Venous thromboembolism is typically seen in sufferers who sustained a venous harm in the course of the exposure. Although rare, ureteral accidents can happen from intraoperative lacerations or ischemia due to direct pressure/stretching from retractor placement. If a particularly troublesome publicity is anticipated with a high threat of such an injury, ureteral stents could be placed to facilitate intraoperative identification of the ureters.
Real Experiences: Customer Reviews on Rumalaya gel
Gancka, 51 years: Once posterior exposure of the spine is finished through careful meticulous subperiosteal dissection, consideration is directed toward placement of instrumentation and subsequent efficiency of osteotomy. Flexion of the hip reduces the quantity of lordosis, will increase the interspinous and interlaminar distances, and facilitates entry to the spinal canal. Neurologic complaints are also extraordinarily uncommon in spondylolysis without spondylolisthesis.
Zuben, 39 years: Thoracic diskectomy is indicated just for sufferers with refractory radicular ache or, more typically, myelopathy. However, a mortality price of up to 40% has been reported in elderly patients placed in a halo vest, maybe on account of respiratory compromise,6 and nonunion rates of as a lot as 41% have also been reported. If a clear tear occurs in the dorsolateral dura, every try ought to be made at a major restore.
Dimitar, 23 years: The preassembled system is superior along the Steinmann pin into the sacrum, across the L5-S1 disk, and into the L5 vertebra. Symptomatic individuals are sometimes older patients, and deformity associated with these lesions Malignant Tumors Primary malignant tumors of the subaxial cervical spine also current with the primary complaint of pain. The superficial fascia is opened, and, using blunt dissection, the aircraft between the sternocleidomastoid muscle and carotid sheath laterally and the trachea and esophagus medially is developed.
Trano, 49 years: Use of a hemostatic matrix down a heavily bleeding pedicle tract should be avoided, as it has been related to fatal embolism. Nausea and vomiting Pump Maintenance the battery lifetime of the programmable pump is estimated at about 5 years. Depending on the clinical state of affairs, the surgeon will determine if sacrifice of the fascicle necessitates a nerve graft restore.
8 of 10 - Review by Z. Grok
Votes: 249 votes
Total customer reviews: 249
References
- Darchia N, Campbell IG, Feinberg I. Rapid eye movement density is reduced in normal elderly. Sleep 2003;26:973-7.
- Nidorf SM, Thompson PL, Jamrozik KD, Hobbs MST. Reduced risk of death at 28 days in patients taking beta-blocker before admission to hospital with myocardial infarction. Br Med J 1990;300:71.
- Thomeer MJ, Costabel U, Rizzato G, Poletti V, Demedts M. Comparison of registries of interstitial lung diseases in three European countries. Eur Respir J Suppl 2001;18:114S-8S. 32.
- Finazzi G, Caruso V, Marchioli R, Capnist G, Chisesi T, Finelli C, et al. Acute leukemia in polycythemia vera. An analysis of 1638 patients enrolled in prospective observational study. Blood 2005;105:2664-70.
- Pomponio RJ, Coskun T, Demirkol M, et al. Novel mutations cause biotinidase deficiency in Turkish children. J Inherit Metab Dis 2000;23:120.
- Hamrahian AH, Ioachimescu AG, Remer EM, et al: Clinical utility of noncontrast computed tomography attenuation value (Hounsfield units) to differentiate adrenal adenomas/hyperplasias from nonadenomas: Cleveland Clinic experience, J Clin Endocrinol Metab 90(2):871n877, 2005.