
Venlafaxine dosages: 150 mg, 75 mg, 37.5 mg
Venlafaxine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase discount venlafaxine on-line
Pain localization Pain from esophagitis, esophageal dysmotility, or esophageal neoplasm usually is substernal and should radiate to the back, jaw, and left shoulder and arm. Small intestinal illness mostly produces periumbilical ache, although ileal lesions may elicit hypogastric signs. Gallbladder and bile duct pain is experienced within the epigastrium and right higher quadrant. Left higher quadrant pain suggests pancreatic illness however may end result from larger curvature gastric ulcers, splenic lesions, perinephric illness, and colonic splenic flexure lesions. Uterine lesions produce midline lower stomach ache, whereas adnexal ache localizes to the ipsilateral decrease quadrant. Cholecystitis could start in the epigastrium and migrate to the right higher quadrant, whereas appendicitis might start in the midline after which move to the McBurney level in the right lower stomach. Pain from small intestinal obstruction or inflammation is colicky or crampy and could additionally be associated with stomach distension and audible bowel sounds. Despite use of the terms biliary colic and renal colic, obstruction of these organs extra often produces a gentle quite than colicky ache. Acute cholecystitis results in squeezing pain, whereas acute pancreatitis ends in penetrating or boring ache. Pain depth Extremely severe belly pain is produced by peptic ulcer perforation, acute pancreatitis, or passage of a renal stone, whereas severe acute pain is evoked by small intestinal obstruction, cholecystitis, and appendicitis. Causes of more moderate acute pain embrace peptic ulcer disease, gastroenteritis, and esophagitis. Intensity of persistent abdominal pain is tougher to assess as a result of psychological components can modify ache perception. Then, oblique questions on interference with sleep or every day function could present helpful information about pain severity. Pain chronology Peptic ulcer ache may be intermittent and sometimes happens within the morning or earlier than meals. Posterior penetration must be thought-about when peptic ulcer pain becomes constant. Acute cholecystitis generally develops during sleep and may be preceded by months of intermittent biliary colic. Nocturnal ache not often happens in patients with irritable bowel syndrome or useful abdominal pain. Appendicitis usually presents as progressive ache for 10�15 hours with out remission. Pain reaching peak depth within minutes is extra attribute of ulcer perforation, abdominal aortic aneurysm rupture, passage of renal stones, or ruptured ectopic pregnancy. In acute pancreatitis, intestinal obstruction, cholecystitis, or mesenteric arterial occlusion, peak ache depth is reached in 10�60 minutes. A gradual onset of ache for hours is reported in appendicitis, some instances of cholecystitis, diverticulitis, and mesenteric venous occlusion. The pain of irritable bowel syndrome is persistent and could additionally be most intense after meals. In girls, pain at month-to-month intervals suggests endometriosis or ovulationrelated signs. Pain after beginning medicine raises the potential of acute intermittent porphyria (barbiturates) or pancreatitis (steroids, tetracycline, thiazides). Alleviating and aggravating factors Antacids or acidsuppressing medications may relieve the ache of esophagitis or peptic ulcer disease. Ingesting meals can relieve discomfort from a duodenal ulcer but could worsen ache because of gastric body ulcers. The pain of pancreatic disease nearly always is intensified by meal ingestion, as is discomfort from the Patient with Abdominal Pain 59 intestinal obstruction or mesenteric ischemia. Duodenal obstruction provokes pain within minutes of eating, whereas ileal lesions trigger pain one to two hours after a meal.
Buy 150 mg venlafaxine with mastercard
Endoscopic injection of botulinum toxin into the pylorus reportedly improves gastric emptying and signs of gastroparesis, presum ably by lowering resistance to outflow into the duodenum. Case stories are promising, however large, longerterm research need to affirm effectiveness. Endoscopic, radiographic, or surgical placement of a gastrostomy tube can pro vide intermittent decompression if the abdomen turns into crammed with gasoline or fluid. Placement of a feeding jejunostomy permits the affected person to continue receiving enteral vitamin when meals ingestion is precluded by extreme nausea and vomiting. In uncommon cases, house complete parenteral vitamin could be given to keep caloric and fluid sustenance. Surgical implantation of a gastric electrical neurostimulator using excessive frequency (12 cycles/minute), lowenergy pulses (not to be confused with "gastric pacing" that employs lowfrequency, highenergy pulses) could reduce Disorders of Gastric Emptying 225 nausea and vomiting in chosen patients with diabetic or idiopathic gastropare sis. Pancreatic transplantation can stabilize the lack of neuronal perform in a patient with severe diabetic complications; furthermore, signs are improved with transplantation. Gastric resection is usually of limited profit, though total gastrectomy reportedly reduces signs specifically in patients with extreme gastroparesis caused by prior vagotomy. Complications and their administration Complications of gastroparesis embrace heartburn from delayed gastric acid clearance, hemorrhage secondary to Mallory�Weiss tears or stasisinduced mucosal irritation, and weight reduction. Bezoar growth might supervene and exacerbate signs of fullness and early satiety. Disorders with Rapid Gastric Emptying Clinical presentation the scientific entity characterized by fast gastric emptying is dumping syndrome, which is essentially a complication of gastric surgical procedure. Early dumping syndrome that occurs within half-hour after ingesting a meal is characterised by bloating, crampy belly pain and diarrhea as well as vasomotor signs corresponding to flushing, palpitations, diaphoresis, lightheadedness, and tachycardia. Late dumping syndrome happens two to three hours after consuming and presents with weak point, palpitations, diaphoresis, tremulousness, confusion, and syncope. Diagnostic investigation the diagnosis of dumping syndrome is predicated on eliciting a characteristic constel lation of symptoms in a patient who has undergone gastric surgical procedure. Differential diagnosis Postsurgical dumping syndrome Any surgical procedure involving gastrectomy or vagotomy may produce the dumping syndrome. The physiology is complicated and variable between patients, however can be ascribed to loss of gastric receptive rest, decreased gastric capability, absence of controlled emptying as a end result of bypass or ablation of the pyloric sphincter, or loss of duodenal suggestions inhibition (in the case of bypassed duo denum in gastrojejunostomy). Early dumping is believed to end result from acceler ated gastric emptying of liquids and fast intestinal filling with hypertonic fluid resulting in fluid shifts and reduction in plasma volume. Late dumping may be attributable to hyperinsulinemic response to the acute carbohydrate load. Liquid emptying may be accelerated in some individuals with duodenal ulcer disease. Many newly diagnosed dia betics have accelerated rather than delayed gastric emptying. Patients with hyperthyroidism might have accelerated emptying, as do some morbidly obese people. Management and prevention Dietary management Dietary suggestions for sufferers with dumping syndrome embrace ingest ing small, frequent meals of foods high in proteins and fats and low in carbohy drates with minimal fluid intake through the meal. Because liquid emptying is more rapid while sitting after vagotomy some sufferers could benefit from lying down (supine) immediately after eating. Medication remedy Octreotide (50�100 mcg subcutaneously half-hour earlier than meals) reduces symp toms of early and late dumping syndrome. Octreotide delays gastric emptying and inhibits the release of enteric hormones and insulin secretion that may cause the symptoms of dumping syndrome. Side results embrace iatrogenic diabetes, malabsorption with worsening of diarrhea and cholelithiasis. Oleic acid may activate the "jejunal brake" and slow intestinal transit and decrease diar rhea in sufferers with dumping syndrome. Surgical remedy Revisional surgical procedure for the dumping syndrome embody RouxenY gastrojejunos tomy, setting up an antiperistaltic jejunal loop between the abdomen and intestine, and retrograde electrical pacing of the small gut. Key apply points the signs of accelerated gastric emptying are usually described as "dumping" syndrome, which has been historically categorized by whether or not signs occur inside half-hour (early) or several hours (late) after meals. Treatment is restricted but consists of dietary changes to smaller, more frequent meals, mendacity down after meals, and octreotide to delay gastric emptying.

37.5mg venlafaxine with mastercard
Characteristics of ischaemic manifestations: Angina and its equal location, duration, depth, precipitating elements, relieving components and related features. These adjustments in medical manifestations are because of sudden and extreme decreases in coronary blood flow due to a lower in coronary artery lumen, consequent to thrombus over underlying atherosclerotic plaque, with or with out superadded spasms. The gold standard for prognosis of coronary ischaemia is growing ranges of metabolic products of ischaemia, importantly lactic acid within the coronary sinus. Patients who had atypical presentation obtained aspirin, heparin and beta-blocker therapy much less aggressively, but there was no distinction in mortality. This acute decrease is secondary to 32 Clinical syndromes in acute coronary syndrome luminal thrombus occurring over a ruptured/eroded atherosclerotic plaque, with a variable element of coronary spasm. The Scientific 100-A Ranking of the Most Influential Scientists, Past and Present. Plaque fissuring: the cause of acute myocardial infarction, sudden ischemic demise, and crescendo angina. National hospital ambulatory medical care survey: 2002 emergency division abstract. Acute chest ache within the emergency room: Identification and examination of lowrisk sufferers. Symptomatic myocardial infarction without chest pain: Prevalence and clinical course. Clinical features of emergency department patients presenting with signs of acute cardiac ischemia: A multicenter examine. Tachycardia and baseline shift are frequent within the acute setting and might make this determination troublesome. The right coronary artery is the only artery that provides the best ventricular free wall (special leads V3R to V6R). Sometimes, nevertheless, partial normalisation may result from the cancellation of opposing vectoral forces. Coronary angiogram revealed complete occlusion of the left anterior descending artery from ostium. There are two patterns of T wave abnormality in Wellens syndrome: Type A: Biphasic, with initial positivity and terminal negativity (25% of cases) Type B: Deeply and symmetrically inverted (75% of cases) the two types of T waves present in Wellens syndrome exist on a spectrum of illness with type-A T waves evolving into type-B T waves. Note deep, symmetrical and inverted T waves in leads V2 and V3, extending up to V5 (type 2 Wellens pattern). Distinguishing the best coronary artery from the left circumflex coronary artery because the infarct-related artery in patients present process main percutaneous coronary intervention for acute inferior myocardial infarction. Electrocardiographic distinction of left circumflex and right coronary artery occlusion in patients with inferior acute myocardial infarction. Electrocardiographic shows of acute complete occlusion of the left major coronary artery. Serious arrythmias incessantly happen and could be deadly earlier than the patient reaches a hospital. In-hospital arrythmias are also a typical cause of morbidity and mortality in these patients [1]. The broken Purkinje fibre cells develop increased automaticity, resulting in re-entrant circuits inside the ventricular myocardium [9]. While extrapolation from animal models to human beings has its limitations, this distinction is likely to be necessary from the therapeutic perspective. The most important technique to cut back incidence of these arrhythmias is timely reperfusion and administration of beta-blockers. Intravenous beta-blocker use has now fallen out of favour after demonstration of increased mortality. Oral beta-blocker therapy, nonetheless, has proven a consistent decrease in mortality in the absence of contraindications [14�16]. The main contraindications for use of beta-blockers are acute cardiac failure as evidenced by low output state, pulmonary congestion or shock, important bradyarrhythmias, and uncontrolled beta-blocker delicate pulmonary illness [16]. Beta-blockers kind the first-line remedy and have been used each alone and as an adjunct with different brokers. Beta-blockers enhance anti-arrhythmic efficacy when used in combination with membrane stabilising agents. It is normally administered as an intravenous bolus followed by infusion which is followed by oral therapy. Wearable cardioverter-defibrillator Wearable cardioverter-defibrillator is a vest-like device worn by the patient beneath the clothing.

Generic venlafaxine 37.5 mg without prescription
Complications of gastrostomies and jejunostomies embrace wound infections, leakage, tube migration, ileus, fever, peritonitis, and necrotizing fasciitis. Parenteral nutrition Potential problems of intravenous nutrition embrace mechanical, infectious, and metabolic issues. Pneumothorax, hemorrhage, brachial plexus damage, air or guidewire embolism, cardiac tamponade, and dying could outcome from 168 Approach to Patients with Gastrointestinal Symptoms or Signs inserting a central venous catheter. Catheters can turn out to be occluded by blood, fibrin, intravenous lipid, or precipitated medication. Vascular catheters are responsible for onethird of nosocomial bacteremias and half of candidemias. Skin flora are the most typical pathogens and embody Staphylococcus aureus, Staphylococcus epidermidis, Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterobacter species, and Candida albicans. Lipid emulsions may cause pulmonary dysfunction, impaired function of the Table 14. Delayed metabolic penalties embody liver dysfunction, bone demineralization, important fatty acid deficiency, and mineral deficiency or excess. Key practice factors � Healthy adults require 20�25 k/kg of body weight to satisfy daily caloric necessities. The patient has been experiencing severe diffuse stomach pain, nausea, and vomiting for the previous forty eight hours. The patient has a historical past of a stricture involving the terminal ileum that required resection two years before. Physical examination demonstrates a diffusely tender abdomen and multiple surgical scars across the stomach. Case 2 A 50yearold man presents to the emergency division with a oneday history of suddenonset severe periumbilical pain, nausea, and vomiting. His labs are notable for a white blood count of 22 K cells/ml, hematocrit of 56%, blood urea nitrogen of 26 mg/dl, amylase 2000 U/l, and lipase of 1947 U/l. He is set to have extreme acute pancreatitis, and early enteral vitamin is initiated by way of a nasojejunal feeding tube. Discussion and potential pitfalls Enteral feeding must be initiated as quickly as extreme acute pancreatitis has been identified as a end result of this has demonstrated decreased infectious problems, decreased hospital days, and a trend toward improving mortality. Benefit has been demonstrated when enteral nutrition is initiated inside 36�48 hours of presentation. Each endoscopic process has a selected set of indications and contraindications. In common, an endoscopic procedure is indicated solely when the outcomes are anticipated to affect the course of affected person management. In some instances, nevertheless, the attendant dangers of endos copy may outweigh the advantages. Before proceeding with endoscopic interven tion, a patient should give a whole historical past and have a complete bodily examination to set up the indication for the examine and exclude the presence of any contraindications. Many procedures require bowel cleaning or extended fasting; subsequently, the clinician should be conscious of comorbid situations, similar to diabetes, coronary heart failure, or renal dysfunction, which can require adjusting the directions for affected person preparation. All patients must be recommended on the dangers and benefits of endoscopy; written and verbal informed consent are obligatory. Principles of average sedation Most endoscopic procedures require reasonable (conscious) sedation to allow a secure and complete examination. The optimal agents and dosages range, but all carry the risk of cardiopulmonary complications. All patients ought to be moni tored for adjustments in blood stress, heart price, and respiratory rate throughout the course of sedation. No digital moni toring can exchange clinical judgment; subsequently, if vital cardiopulmonary indicators or symptoms arise, the procedure must be aborted. Slow titration of the initial dose of the sedative agent is one of the only ways to keep away from oversedation. Antibiotic prophylaxis the position of preprocedure antibiotics to forestall endocarditis or bacteremia in patients with vascular or other prostheses is undefined. Based on the docu mented risks of bacteremia with given procedures and the dangers of building an infection in sure preexisting situations, the American Society of Gastrointestinal Endoscopy offers pointers for antibiotic prophylaxis earlier than endoscopic procedures (Table 15. Antibiotics may be pricey, and heaps of have a substantial danger of allergic reactions. These issues have to be considered when considering using prophylactic antibiotics.

Best buy for venlafaxine
Prevalence of autism spectrum disorders � Autism and Developmental Disabilities Monitoring Network, United States, 2006. Prenatal valproate exposure and threat of autism spectrum problems and childhood autism. Studies on the role of intercourse steroids within the suggestions management of gonadotropin concentrations in men. Testosterone modulation of seizure susceptibility is mediated by neurosteroids 3alpha-androstanediol and 17beta-estradiol. Sex hormones, sexual exercise and plasma anticonvulsant ranges in male epileptics. Differential results of antiepileptic medicine on sexual operate and hormones in males with epilepsy. Epilepsy syndrome, focus location, and remedy selection affect testicular operate in men with epilepsy. Management issues for women with epilepsy � concentrate on being pregnant (an evidence-based review): teratogenesis and perinatal outcomes. Report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society. No enchancment was noted when used for absence, atonic, tonic, and myoclonic seizures. Ethosuximide was efficient for absence seizures, but not focal-onset or tonic�clonic seizures. The introduction of valproate within the 1960s in Europe and in 1978 in the United States dramatically improved the ability to control these seizures. Many introduced new mechanisms of action, pharmacokinetic properties, and improved safety or tolerability. In testing, brivaracetam was found to have proportionally higher antiseizure efficacy in animal fashions with audiogenic seizures. It additionally surpassed levetiracetam in its capacity to exert safety towards seizures induced in normal animals by electroshock therapy and several other chemoconvulsants, together with Metrazol threshold testing. Therefore, subsequent studies discovered brivaracetam to also exhibit some inhibitory exercise on neuronal voltage-gated sodium channels. Pharmacokinetics were just like levetiracetam with little protein binding, intensive renal metabolism, and renal elimination. However, such issues had been also not outstanding in early trials of levetiracetam, so a longer interval of statement may be needed. No major organ toxicity has been reported, and pores and skin hypersensitivity has been rare. Brivaracetam is presently out there in 50 mg tablets and in liquid kind, in addition to in parenteral kind. In the Nineteen Fifties, Geigy, a pharmaceutical company in Switzerland, developed carbamazepine seeking a neuroleptic similar to chlorpromazine. The drug was tested in Europe in the 1960s for the remedy of symptomatic epilepsy with focal and generalized tonic�clonic seizures. Carbamazepine is nearly fully metabolized within the liver, with solely about 5% excreted unchanged. Carbamazepine stimulates the transcriptional upregulation of genes, concerned in its own metabolism, via a strategy of autoinduction. As days and weeks go on, the liver turns into more able to metabolizing the drug, and a steady dose of 600�800 mg/day or more may be taken and simultaneously eradicated. Certain medicines taken for high blood pressure, as nicely as antibiotics corresponding to erythromycin, can interfere with the clearance of carbamazepine and trigger it to construct up in the blood, causing adverse results. Effectiveness has been extensively studied in trials in giant numbers of sufferers. Overall, carbamazepine produces complete control of tonic�clonic seizures in approximately 80% of sufferers. Success with treating focal seizures is somewhat much less, with only two-thirds being fully controlled. Although carbamazepine is nicely tolerated by most people, adverse results can arise, notably upon initiation. It might trigger sleepiness, dizziness, stomach upset, and blurred or double imaginative and prescient, particularly inside the first few days. First, the mind must develop tolerance to the drug and this will likely take per week or two, although typically it takes only some days.
Buy venlafaxine 37.5mg with visa
A 66-year-old lady with genetic generalized epilepsy (juvenile myoclonic epilepsy). The spike�wave discharges may be seen with greater amplitude within the fronto-central leads, and should turn into extra outstanding with eye closure, hyperventilation (which typically triggers an actual seizure with scientific signs), drowsiness, and hypoglycemia. At times, the spike�wave frequency may be initially sooner, round four Hz, and slows barely towards the end. Occurrence of generalized epileptiform discharges in some cases can have genetic predisposition that will or could not progress to the scientific seizures. The generalized spike-and-slow-wave morphology can seem extra fragmented, and sometimes has an initial polyspike component demonstrating up to eight subsequent waveforms. A photoparoxysmal response characterised by bilateral and synchronous polyspike or polyspike-and-slow-wave discharges may be seen in these sufferers with photic stimulation, frequently with greater flash frequencies in the 12�20 Hz vary. The discharges will not be time locked to the flash frequency, and can even happen after the flash stimulus has been terminated. The spike component specifically can appear broader with an extended length, in keeping with a pointy wave rather than a spike. These sufferers are often cognitively delayed due to perinatal mind insult or de novo genetic mutation, and may have structural abnormalities on imaging studies. They typically carry a analysis of Lennox�Gastaut syndrome, though, this is solely one of many potential clinical syndromes during which this sample occurs. This was first outlined by Gibbs and Gibbs in 1952, and was described as "random high-voltage waves and spikes. At times they appear to be focal, and some seconds later they seem to originate from a number of foci. Occasionally the spike discharge turns into generalized, but it by no means appears as a rhythmically repetitive and extremely organized pattern that could be confused with a discharge of a petit mal or petit mal variant kind. This sample is basic for infantile spasms, which are seen in very young patients (aged 4 months to four years old), who usually exhibit significant cognitive delay. Tuberous sclerosis is a standard etiology, but hypsarrhythmia can even produce other infectious, metabolic, or genetic causes. The hypsarrhythmia sample evolves over time as the affected person ages due to progressive myelination and synaptogenesis. This sample can be seen in generalized epilepsies with distinguished tonic seizures, and can happen in combination with a diffuse electrodecrement of the background activity. Electrodecrement is an ictal sample seen with the tonic and atonic seizures in symptomatic generalized epilepsies. A 56-year-old girl with genetic generalized epilepsy (juvenile myoclonic epilepsy). Ictal offset could also be abrupt or gradual, and is usually followed by diffuse background attenuation and diffuse high-amplitude delta-range slowing. Asymmetry of the postictal slowing is an indication of increased cerebral dysfunction in the involved hemisphere, and could additionally be useful in lateralizing the seizure onset. The onset sample of partial seizures in scalp recordings might be seen as sinusoidal waves, repetitive discharges corresponding to spikes and sharp waves, or an electrodecremental response. Rhythmic 5�9 Hz activity is a common sample seen inside the first 30 s of a seizure this has been reported with greater frequency in mesial temporal lobe seizures � as a lot as 65�90% when localized to the temporal leads,37�40 � and much more regularly in sufferers with advanced hippocampal atrophy � as much as 79%. Neocortical temporal lobe epilepsy may exhibit slower 2�5 Hz, rhythmic or polymorphic, and irregular exercise on the onset of seizures. The aforementioned bilateral synchrony can be seen incessantly due to deep epileptogenic focus and speedy generalization. There may be delicate findings corresponding to rhythmic slowing or background attenuation preceding or following the seizure. Electrical decrement or attenuation seen on the onset of seizures is often a very refined discovering that marks the start of a seizure. This is seen as an abrupt suppression that disrupts the background exercise briefly prior to more obvious ictal activity, which may be seen focally, involving only a few electrodes. Otherwise, the background attenuation could also be diffuse and, though useful in figuring out seizure onset, has no localizing or lateralizing value. Sudden cessation of beforehand recurring interictal discharges can also mark the onset of a seizure.

Order venlafaxine
More common in uncontrolled hypertension, female intercourse, previous historical past of stroke and low physique weight [18]. Long-term good thing about major angioplasty as compared with thrombolytic remedy for acute myocardial infarction. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: A quantitative evaluate of 23 randomised trials. Long distance transport for primary angioplasty vs quick thrombolysis in acute myocardial infarction. A comparability of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. Mortality and prehospital thrombolysis for acute myocardial infarction: A meta-analysis. An international randomized trial evaluating four thrombolytic strategies for acute myocardial infarction. The primary aim of early anti-coagulation is to scale back the ischaemic burden within the myocardium with out increasing the haemorrhagic events. Research is ongoing to determine the function of long-term anti-coagulants to stop subsequent coronary occasions once the acute stage is over. Heparin requires parenteral administration and is usually given via a continuous intravenous route. Levels of heparin-binding proteins differ from person to particular person inside the blood circulation, which finally ends up in unpredictable and variable anti-coagulant responses of heparin. Rupture of the plaques leads to activation of platelets and coagulation cascade on account of harm to blood vessels. It has also been postulated that heparin discontinuation causes organic rebound technology of thrombin and increases prothrombotic state [4]. The most typical facet effect is bleeding, and the antidote protamine can be used in patients with critical bleeding. It has higher bioavailability, predictable anti-coagulant response and longer half-life than heparin. Doses have to be lowered in renal dysfunction and monitoring of anti-coagulant effects is indicated in special teams of patients corresponding to those who are pregnant and in presence of mechanical prosthetic valves. Because of its renal clearance, it should be given cautiously to patients with renal dysfunction and must be prevented when creatinine clearance is lower than 20 mL/min. The solely indication of warfarin is in patients requiring triple therapy (anti-coagulant and twin anti-platelet therapy), similar to patients with atrial fibrillation, mechanical valves or deep venous thromboembolism. There is want of early and environment friendly anti-coagulation therapy to block the coagulation cascade and prevent ischaemic injury to the myocardium. However, sufferers within the bivalirudin group were discovered to have a four-fold increase in acute stent thrombosis. Three teams had similar ischaemic outcomes however main bleedings were reduced in the bivalirudin group. Rivaroxaban decreased main ischaemic outcomes together with death, myocardial infarction or stroke however at the worth of elevated bleeding in dose dependent method. This trial was different as rivaroxaban was used in place of aspirin, not concurrently. However, it was associated with important three-fold increase in catheter and periprocedural thrombosis. It is limited to therapy throughout preliminary hospitalisation and revascularisation at current. A patient-centric approach ought to be followed to stability ischaemic and bleeding dangers. Clinical results of anticoagulant therapy in suspected acute myocardial infarction: Systematic overview of randomised trials. Part 9: Acute coronary syndromes: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations.
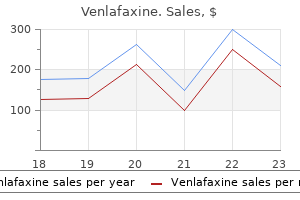
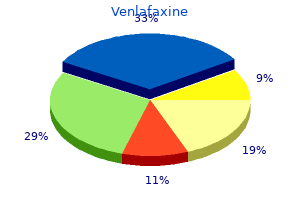
Real Experiences: Customer Reviews on Venlafaxine
Cyrus, 38 years: They characteristically decompress with elevation and native compression and enlarge on Valsalva maneuver. Dual anti-platelet therapy (aspirin plus a P2Y12 inhibitor) should be used for 12 months for all sufferers [44].
Navaras, 60 years: Serum cytokine profiles are altered in patients with progressive infantile hemangioma. This useful effect was impartial of type and dose of cardiac rehabilitation in addition to trial publication date.
Karmok, 43 years: The diagnostic prospects are amplified by the continual evolution of the imaging methods. Nodular regeneration and fibrosis within the area of Disse improve postsinusoidal and sinusoidal resistance, respectively.
8 of 10 - Review by S. Kapotth
Votes: 183 votes
Total customer reviews: 183
References
- Eide K, Torjesen PA, Drolsum A, et al. Low-renin status in therapy resistant hypertension: a clue to efficient treatment. J Hypertens 2004;22:2219-2226.
- Renehan AG, Tyson M, Egger M, et al. Body-mass index and incidence of cancer: a systematic review and metaanalysis of prospective observational studies. Lancet 2008;371(9612):569-578.
- Fox M, Power RF, Bruce AW: Diverticulum of the bladderopresentation and evaluation of treatment of 115 cases, Br J Urol 34:286n298, 1962.
- Birnbaum BF, Pinzone JJ: Sickle cell trait and priapism: a case report and review of the literature, Cases J 1:429, 2008.
- El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 2012;142(6):1264- 1273.
- Trevelyan, S. L., Carlson, G. L. Is TNP in the open abdomen safe and effective? J Wound Care. 2009; 18:24-25.