
Gabapentin dosages: 800 mg, 600 mg, 400 mg, 300 mg, 100 mg
Gabapentin packs: 30 pills, 60 pills, 90 pills, 180 pills, 120 pills, 270 pills, 360 pills

Purchase gabapentin 100 mg with mastercard
Solutions to the inverse problem involve simplifications and approximations and, even when well-defined dipoles using implanted sources in the human brain are employed, often produce errors of a few centimeters (120,121). Although it is not possible to uniquely identify the positions of the electrical sources in the brain from the scalp electrodes (122), appropriate assumptions can yield useful information in some cases (16,123). An illustration of the practical use of the equivalent current source dipole method to localize an epileptic discharge is shown in Figure 7. Localization using dipole source analysis has been the subject of many validation (124) and comparison studies (125). In recent years, purveyors of these packages have enhanced their offerings to be of more use in clinical medicine. Several journals have dedicated special issues to the various aspects of this methodology (126). Although computerized "source analysis" was applied beginning in the mid-1980s to identify single or multiple foci (117,118), and has been continuously developed for more than 20 years, the extra time and effort required have discouraged use of these techniques on a routine basis. This software methodology is sometimes limited, because in clinical use only the simplest of models of the source. The temporal dynamics of the source and the intracranial anatomic pathology associated with epilepsy often make these models inexact, and the results may be misleading (127). The volume conductor model that represents the physical properties of the medium between the sources and the sensors is especially complex for the electroencephalography of patients with highly distorted head anatomy. Ueber einige Gesetze der Vertheilung elektrischer Strome in korperlichen Leitern mit Anwendung. Clinical ictal patterns in epileptic patients with occipital electroencephalographic foci. Occipitotemporal epilepsy studied with stereotaxically implanted depth electrodes and successfully treated by temporal resection. Measurement of the conductivity of skull, temporarily removed during epilepsy surgery. Influence of tissue resistivities on neuromagnetic fields and electric potentials studied with a finite element model of the head. A hole in the skull distorts substantially the distribution of extracranial electrical fields in an in vitro model. Epidural pegs and foramen ovale electrodes: a new class of electrodes of intermediate invasiveness for the mapping of seizure foci. Localization of epileptogenic spike foci: comparative study of closely spaced scalp electrodes, nasopharyngeal, sphenoidal, subdural, and depth electrodes. Commentary: chronic intracranial recording and stimulation with subdural electrodes. Subdural electrodes in the evaluation for epilepsy surgery in children and adults. Comparison of subcortical, cortical and scalp activity using chronically indwelling electrodes in man. Neuronal generators and the problem of localization in electroencephalography: application of volume conductor theory to electroencephalography. Bipolar, unipolar and average reference recording methods, I: mainly theoretical considerations. Design and evolution of a system for long-term electroencephalographic and video monitoring of epilepsy patients. Simultaneous intracranial and extracranial recording of interictal epileptiform activity in patients with drug resistant partial epilepsy: patterns of conduction and results from dipole reconstructions. Electrode montages and localization of potentials in clinical electroencephalography. Spatiotemporal relationship between seizure activity and interictal spikes in temporal lobe epilepsy. Configuration and laminar analysis of the "resting" potential gradient, of the main transient response to perforant path, fimbrial and mossy fiber volleys and of "spontaneous" activity. Comparison and correlation of surface and sphenoidal electrodes with simultaneous intracranial recording: an interictal study. Generation of scalp discharges in temporal lobe epilepsy as suggested by intraoperative electrocorticographic recordings. Analysis of the electromagnetic signals of the human brain: milestones, obstacles, and goals.
Cheap gabapentin 300mg otc
It is intended for internal use only and should be disseminated only to authorized recipients. The contents of the therapeutic class overviews on this website ("Content") are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Patients should always seek the advice of a physician or other qualified health provider with any questions regarding a medical condition. Clinicians should refer to the full prescribing information and published resources when making medical decisions. The most frequently reported adverse events with glatiramer acetate include a transient, self-limiting, post-injection systemic reaction immediately following drug administration consisting of flushing, chest pain, palpitations, anxiety, dyspnea, throat constriction, and urticaria. Glatiramer acetate does not have any known drug interactions and is not associated with an increased risk of hepatotoxicity or depression. Therefore, patients experiencing an inadequate response or druginduced adverse event should be switched to a different biologic response modifier (Coyle 2008, Portaccio et al 2008). There are now 3 available oral agents: Gilenya (fingolimod), which was approved in 2010, Aubagio (teriflunomide), which was approved 2012, and Tecfidera (dimethyl fumarate), which was approved in 2013. Among other potential benefits, it is expected that the availability of oral agents may increase convenience and improve patient adherence to their drug regimen (Sanvito et al 2011). The available oral drugs each have different mechanisms of action and tolerability profiles. The oral products have not been compared to one another in any head-to-head trials. The adverse event profile for fingolimod includes cardiovascular risks including bradycardia. Isolated delayed events, including transient asystole and unexplained death, have occurred within 24 hours of the first dose. Gastrointestinal intolerance and flushing are common side effects that may wane with time; slow titration to maintenance doses, taking the medication with food, and premedication with aspirin may reduce their severity. Aubagio (teriflunomide) inhibits dihydroorotate dehydrogenase, a mitochondrial enzyme involved in de novo pyrimidine synthesis. Teriflunomide has boxed warnings for the possibility of severe liver injury and teratogenicity. It is intended for internal use only and should be disseminated only to authorized recipients. The contents of the therapeutic class overviews on this website ("Content") are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Patients should always seek the advice of a physician or other qualified health provider with any questions regarding a medical condition. Clinicians should refer to the full prescribing information and published resources when making medical decisions. The convenient dosing schedule of 2 annual treatment courses is counterbalanced by the need for regular monitoring of the increased risk for autoimmunity. As a humanized form of Rituxan (rituximab), ocrelizumab is expected to be less immunogenic with repeated infusions and may have a more favorable benefit-to-risk profile than Rituxan (Sorensen et al 2016). Short- and long-term clinical outcomes of use of beta-interferon or glatiramer acetate for people with clinically isolated syndrome: a systematic review of randomised controlled trials and network meta-analysis. Decisional Dilemmas in Discontinuing Prolonged Disease-Modifying Treatment for Multiple Sclerosis. Clinical course after change of immunomodulating therapy in relapsing-remitting multiple sclerosis. It is intended for internal use only and should be disseminated only to authorized recipients. The contents of the therapeutic class overviews on this website ("Content") are for informational purposes only.
Diseases
- Albinism immunodeficiency
- Bazopoulou Kyrkanidou syndrome
- Brachycephaly deafness cataract mental retardation
- Achalasia, familial esophageal
- Capos syndrome
- 3-hydroxyacyl-coa dehydrogenase deficiency
- Kearns Sayre syndrome
- MASA syndrome
- Pierre Robin sequence congenital heart defect talipes
Purchase gabapentin on line amex
Over-the-counter analgesic medications can be present in or components of common cold and cough medicine; clinicians must ensure that patients are aware of and discuss all their medications with their doctor or pharmacist. Risks of acetaminophen include dose-dependent liver toxicity, especially when the drug is taken at high doses, with alcohol, or by those with liver disease. Anticonvulsants are medications originally developed to treat seizures, but they are also commonly used to treat different pain syndromes, including postherpetic neuralgia, peripheral neuropathy, and migraine. Some of these agents can effectively treat the neuropathic components of pain syndromes. Anticonvulsants, which include gabapentinoids such as gabapentin and pregabalin, may cause significant sedation and have recently been associated with a possible risk of misuse. As with other medications, they have risks and adverse effects, including dry mouth, dizziness, sedation, memory impairment, orthostatic hypotension, urinary retention, and cardiac conduction abnormalities. There have been some reports of withdrawal reactions when these medications are suddenly stopped. Overall, the analgesic actions of antidepressants occur even in patients who are not clinically depressed, and their analgesic effect typically occurs sooner and at lower doses than those required for the treatment of depression. Carisoprodol is metabolized to meprobamate, which is both sedating and possibly addictive, so the use of carisoprodol is not recommended, particularly because alternatives are available. Benzodiazepines do not have independent analgesic effects but may have indirect pain-relieving effects. Second, co-prescription of benzodiazepines and opioids is associated with enhanced risks of overdose, respiratory depression, and death. For more severe cases of co-morbid anxiety disorders, psychiatric consultation for medication regimens is advised. It should be noted that gabapentinoids have been useful in treating anxiety in patients with pain. Opioids are a controlled substance group of broad-spectrum analgesics that provide pain relief for a variety of conditions. Administration of opioid medication can include short- or long-acting formulations104 and different delivery modalities, such as oral, buccal, sublingual, spray, intravenous, intramuscular, intrathecal, suppository, transdermal patches,105 and lozenge formulation. Opioids bind to opioid receptors in the brain, spinal cord, and other sites, activating analgesic and reward pathways. Illicit fentanyl-related overdoses are now a leading cause of deaths from overdose in the United States, often because of its use in combination with alcohol or illicitly obtained heroin, cocaine, diverted prescription opioids, and other drugs such as benzodiazepines. Common prescription opioid medications that can be considered for management of acute and chronic pain include hydromorphone, hydrocodone, codeine, oxycodone, methadone, and morphine. In some states, there is a significant challenge, however, for prescribing clinicians to get authorization for using buprenorphine for chronic pain management (see Section 2. Opioid treatment should be maintained for a period no longer than necessary for adequate pain control. Much of the risk at higher doses appears to be associated with co-prescribed benzodiazepines. They just look at us as another number or as those patients coming in seeking drugs. But I also do other things- vitamins, try to eat healthy, try not to be stressed out- just all sorts of things to help myself. But the main thing is, we need opioid medications to be an option in the tool box. Medicines play an important role in treating certain conditions and diseases, but they must be taken with care and stored securely where they cannot be misused by a third party or accidentally ingested by children or pets. Patients and caregivers can remove expired, unwanted, or unused medicine from their home as soon as they are no longer needed to help reduce the chance that others accidentally or intentionally misuse the unneeded medicine and to help reduce drugs from entering the environment. The illicit fentanyl analogues used are not necessarily the same product that is legally prescribed and used during surgeries or in the transdermal and mucosal fentanyl preparations provided for moderate to severe pain. One illicit analogue that has been seen is called carfentanil, which is 100 times more potent than fentanyl. The availability of naloxone as well as patient and family education about naloxone can mitigate the risks of fentanyl-related overdose.

Buy generic gabapentin pills
Aphasic seizures are seizures with predominant dysphasia or aphasia and preserved consciousness. Atonic seizures involve loss of postural tone, resulting in head drops or limp falling. Videopolygraphic studies show that these may be caused by pure atonia, atonia following a myoclonic jerk, or pure tonic stiffening, but in clinical practice, the exact pathogenesis is often unclear. Hypomotor seizures are characterized by decreased or absent behavioral motor activity without the emergence of new motor manifestations; this descriptive term is only needed for infants or severely mentally impaired individuals, in whom it is not possible to test consciousness directly (16,30). Akinetic seizures are characterized by the inability to perform voluntary movements despite preserved consciousness, as may occur with activation of the negative motor areas in the mesial frontal and inferior frontal gyri. Negative myoclonic seizures consist of a brief (50 to 200 msec) interruption of tonic muscle activity caused by an epileptiform discharge; the resulting brief, sudden movement is caused by loss of muscle tone. Modifiers may be added to classify the somatotopic distribution of ictal signs and symptoms, as, for example, "lefthand clonic seizure" or "generalized clonic seizure. To express the evolution of symptoms that occurs as the seizure discharge spreads to new cortical areas, the components can be listed in order of appearance and linked by arrows (see examples below). Precise definitions of the state of consciousness is necessary only for some specific seizure types, such as dialeptic seizures, in which loss of consciousness is the predominant symptom, and auras, in which consciousness is always preserved. There are several semiological features of the ictal or postictal state that are not necessarily the main element of a seizure component, but have been established as reliably lateralizing the hemisphere of seizure onset-for example, dystonic posturing (31), ictal speech (32), or postictal weakness (33). These lateralizing signs can be listed following the seizure sequence (see example below). If information is limited, as in the absence of a witness or a complete or accurate history, a less detailed classification may be appropriate. Progressively greater amounts of information may permit further categorization of the seizure as "simple motor seizure," "right arm motor seizure," or "right arm clonic seizure. Thus, important information may be preserved and misclassification (or no classification at all) may be prevented. This proposal uses the strictly descriptive terminology of the semiological seizure classification, but categorizes it as a glossary (29). The second axis contains the epileptic seizure types "that present diagnostic entities with physiologic, therapeutic, and/or prognostic implications" (34). Regardless of the seizure classification system that is used, one must bear in mind that in every case, the seizure classification must be complemented by an epilepsy classification that specifies the etiology of the epilepsy, the location of the epileptogenic zone, and other important medical or neurological conditions the patient has. Commission on Classification and Terminology of the International League Against Epilepsy. Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Classifications of the International League Against Epilepsy: time for reappraisal. An analysis of clinical seizure patterns and their localizing value in frontal and temporal lobe epilepsies. Lateralizing value and semiology of ictal limb posturing and version in temporal lobe and extratemporal epilepsy. Of cabbages and kings: do we really need a systematic classification of epilepsies Of cabbages and kings: perspectives on classification from the field of systematics. Reply to "Of cabbages and kings: some considerations on classifications, diagnostic schemes, semiology, and concepts".
Discount 100mg gabapentin visa
The time of onset of efficacy is an important consideration in the choice of antiepileptic medication. Lacosamide in fixed doses of 200, 400, or 600 mg/day were used in these pooled data. Titration was started at 100 mg/day during the initial week of lacosamide exposure, followed by weekly titration in 100-mg increments to the assigned target dose. After the first week of lacosamide exposure to 100 mg/day, the percent reduction of seizures over placebo was 17. Post hoc pooled analysis showed an early onset of efficacy starting at a dose of 100 mg/day in the first week and increasing modestly after that for patients where lacosamide was added to their antiepileptic medication regimen. Thus, efficacy can be expected in the first week or two following initiation of adjunctive lacosamide. Clinical use suggests that lacosamide be initiated as an adjunctive at 50 mg twice daily with subsequent dose increases on a weekly basis to a target dose of 200 to 400 mg/day in adults with partial epilepsy. The availability of a parenteral formulation has the potential to be useful in the management of acute seizures, although, studies in status epilepticus are still to be performed. Studies in other populations, including pediatrics and the elderly, are needed to further define the therapeutic spectrum of lacosamide. Studies in Diabetic Neuropathy At least three randomized, placebo-controlled, double-blind trials have been completed to test the efficacy of lacosamide in diabetic neuropathy related pain. However, doses of 600 mg/day were not associated with further increments in efficacy and were generally less well tolerated (10). Oral administration of lacosamide results in rapid and near complete absorption with minimal first-pass effects (12). Bioavailability after oral administration approaches 100%, with peak plasma concentration being reached after 30 min to 4 hours following oral administration. Dose to plasma concentrations are linear with low intra- and intersubject variability. Escalating dose administration orally results in near-linear increases in serum concentration. Lacosamide administered in a 300-mg single dose following consumption of a high fat diet did not influence its serum concentration. Distribution in placenta and breast milk and distribution in children has not been examined. A further 30% is metabolized by demethylation to the pharmacologically inactive O-desmethyl metabolite that is excreted in the urine (14). As a class, inducer antiepileptic medications increased clearance by approximately 36%. The observed effect of inducer antiepileptic medications on lacosamide exposure was modest. Accordingly, this finding is unlikely to be clinically significant when adding lacosamide to an existing treatment regimen. When used at therapeutic concentrations, lacosamide did not have a significant effect on the cytochrome P450 enzyme system. Human hepatocyte showed no potential to induce cytochrome P450 isoforms including 1A2, 2B6, 2C9, 2C19, and 3A4. The dosage at which this inhibition would be expected is unlikely to be routinely achieved in the treatment of human epilepsy. Generally, lacosamide was well tolerated when combined with up to three concomitant antiepileptic medications. Intravenous Administration Intravenous administration of lacosamide was studied in a multicenter, double-blind, double-dummy, randomized, inpatient trial evaluating the safety, tolerability, and pharmacokinetics as replacement for oral lacosamide (18). This study utilized patients from an open-label extension trial of oral lacosamide and randomized to either intravenous lacosamide and oral placebo or intravenous placebo and oral lacosamide. Treatment-emergent adverse events were mild and included dizziness, headache, back pain, somnolence, and injection site pain and were similar to oral lacosamide. There were no significant cardiac/hemodynamic adverse effects noted and there does not appear to be the need for special monitoring of cardiovascular function. Efficacy of the intravenous formulation in partial complex seizures or status epilepticus has not been studied. This is not surprising given the very recent availability of an intravenous formulation.
Purchase gabapentin discount
Missed Doses Counsel patients that if they miss a dose, they should resume dosing the following day at their prescribed daily dose. Instruct patients to contact their physician if more than one day of dosing is missed. If you have suicidal thoughts or actions, your healthcare provider may check for other causes. Call your healthcare provider between visits as needed, especially if you are worried about symptoms. You may have problems walking normally if you are unsteady because you feel dizzy. Your risk of feeling dizzy and having problems walking normally may be higher if you are elderly. Call your healthcare provider right away if you have: o a skin rash, hives o f ever or swollen glands that do not go away o swelling of your face o shortness of breath, swelling of the legs, yellowing of the skin or whites of the eyes, or dark urine. Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Active ingredient: perampanel Inactive ingredients (tablets): lactose monohydrate, low substituted hydroxypropyl cellulose, povidone, microcrystalline cellulose, magnesium stearate, hypromellose, polyethylene glycol, talc, and titanium dioxide. Inactive ingredients (oral suspension): sorbitol, microcrystalline cellulose, carboxymethylcellulose sodium, poloxamer, simethicone, citric acid, sodium benzoate, and purified water. This leaflet does not take the place of talking to your healthcare provider about your medical condition or treatment. Uncap the bottle and insert the bottle adapter into the bottle by pressing downward. Push the plunger of the syringe all the way down then insert the syringe into the upright bottle through the opening in the bottle adapter. Pull the plunger to withdraw the dose prescribed by your healthcare provider (the amount of liquid medicine in Step 4). If you see air bubbles in the oral syringe, fully push in the plunger so that the oral solution flows back into the bottle. If the dose is more than 20 mL, repeat Steps 4 through 6 when drawing up the remaining dose of medicine. If you need 2 syringes for the dose, slowly squirt the medicine from the first syringe into the mouth, then slowly squirt the medicine from the second syringe into the mouth. Of the 150,000 new cases of epilepsy diagnosed each year, approximately 50,000 of these cases will be diagnosed in children and adolescents under the age of 18. About two-thirds of all children with epilepsy outgrow their seizures by the time they are teenagers. The goal of eliminating seizures while preventing side effects is achievable for most children and youth, but it requires an organized system of care to ensure uniformity in the provision of services and support. As a parent, you want to help your child maintain a healthy lifestyle and ensure he/ she has regular medical visits. How to Use this Toolkit the toolkit is organized into six sections-About Epilepsy, Managing Epilepsy, Daily Life with Epilepsy, Life Stages with Epilepsy, Resources and Forms. Each section includes information and helpful tips with links to downloadable tools. You can either check the Table of Contents at the front of this document for specific information, or see the reference sections on the front of each tab. This will not only help your doctor, but also make you feel more organized and in control. If you would like to find out about all the resources available from the Epilepsy Foundation, visit Clusters of nerve cells, or neurons, in the brain sometimes signal abnormally and cause a person to have seizures.
Decalepis hamiltonii (Swallowroot). Gabapentin.
- Are there any interactions with medications?
- What is Swallowroot?
- Dosing considerations for Swallowroot.
- Stimulating appetite.
- Are there safety concerns?
- How does Swallowroot work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97085
Purchase gabapentin with american express
Positive prediction value regarding seizure freedom was 78% and negative predictive value was 64% for these cases. They found no statistical differences regarding overlap of epileptogenic regions identified by each of the both methods with the resection zone. However, some methodical limitations have to be considered, mainly the sampling bias of some invasive recordings performed with only few depth electrodes. Reduction of both, the total number of invasive recordings and the number or insufficient invasive evaluations due to false electrode positions or incomplete coverage of the epileptogenic zone, seems a realistic goal. Electromagnetic source analysis adds information to the localization and organization of both, epileptogenic and normal cortical areas, which turns out to be clinically relevant in at least 10% of the cases. In addition, the impact of electromagnetic source analysis in the prediction of postsurgical seizure outcome has to be further investigated. Magnetoencephalography: evidence of magnetic fields produced by alpha rhythm currents. Interictal electromagnetic source imaging in focal epilepsy: practices, results and recommendations. Modality-specific spike identification in simultaneous magnetoencephalography/electroencephalography: a methodological approach. Functional organization of the human first and second somatosensory cortices: a neuromagnetic study. Magnetoencephalography: theory, instrumentation and applications to noninvasive studies of the working human brain. Demonstration of useful differences between magnetoencephalogram and electroencephalogram. Magnetoencephalography in partial epilepsy: clinical yield and localization accuracy. Detection of epileptiform activity by human interpreters: blinded comparison between electroencephalography and magnetoencephalography. Magnetoencephalographic spikes not detected by conventional electroencephalography. Magnetoencephalography is more successful for screening and localizing frontal lobe epilepsy than electroencephalography. Feasibility and limitations of magnetoencephalographic detection of epileptic discharges: simultaneous recordings of magnetic fields and electrocorticography. Interictal and ictal magnetoencephalographic study in patients with medial frontal lobe epilepsy. Single and multiple clusters of magnetoencephalographic dipoles in neocortical epilepsy: significance in characterizing the epileptogenic zone. Magnetic source imaging versus intracranial electroencephalogram in epilepsy surgery: a prospective study. Anatomical correlates for magnetoencephalography: integration with magnetic resonance images. Source localization determined by magnetoencephalography and electroencephalography in temporal lobe epilepsy: comparison with electrocorticography: technical case report. Multiple source analysis of interictal spikes: goals, requirements and clinical value. Application of magnetoencephalography in epilepsy patients with widespread spike or slow-wave activity. Magnetoencephalographic evaluation of children and adolescents with intractable epilepsy. Utility of magnetoencephalography in the evaluation of recurrent seizures after epilepsy surgery.
Cheap 300mg gabapentin with mastercard
Source: Toluene is an aromatic hydrocarbon, occurring naturally in crude oil and in the tolu tree. It is produced during the process of making gasoline and other fuels from crude oil, in making coke from coal, and as a by-product in the manufacture of styrene. Toluene has numerous commercial and industrial applications and is a solvent in paints, lacquers, thinners, glues, correction fluid and nail polish remover, and is used in the printing and leather tanning processes. Recreational use is most common among younger adolescents primarily because it is readily available, inexpensive and legal. Potency, Purity and Dose: Solvents in many commercial and industrial products are often mixed and the solvent "sniffer" is often exposed to other solvents in addition to toluene. Acute and chronic accidental exposure to toluene can also occur, particularly in work environments. May be sniffed directly from on open container, or "huffed" from a rag soaked in the substance and held to the face. Alternatively, the open container or soaked rag can be placed in a bag where the vapors can concentrate before being inhaled. Pharmacokinetics: Toluene is well-absorbed following oral ingestion and rapidly absorbed following inhalation. Toluene is detectable in the arterial blood within - 85 - 10 seconds of inhalation exposure. It is highly lipid soluble and accumulates in adipose tissue, tissues with high fat content, and highly vascularized tissues. Side-chain hydroxylation to benzyl alcohol is followed by oxidation to benzaldehyde by alcohol dehydrogenase, oxidation to benzoic acid by aldehyde dehydrogenase and conjugation with glycine to hippuric acid or reaction with glucuronic acid to form benzoyl glucuronide. Molecular Interactions / Receptor Chemistry: Toluene is metabolized to benzyl alcohol via the cytochrome P450 2E1 isoform, and to a lesser extent to benzyl alcohol, o-cresol, and p-cresol by 2B6, 2C8, 1A2 and 1A1 isoforms. Potential inhibitors of these isoenzymes could decrease the rate of toluene elimination if administered concurrently, while potential inducers could increase the rate of elimination. Blood to Breath Concentration Ratio: Ranges from 7 to 15 Interpretation of Blood Concentrations: In non-exposed individuals, average toluene concentrations have been measured at 0. Similarly, exposure to 34 ppm for 8 hours resulted in blood toluene concentrations of 0. In 136 toluene abusers hospitalized or arrested while intoxicated, blood toluene concentrations ranged from 0. Three fatalities from acute toluene inhalation had blood concentrations of 50, 60, and 79 mg/L. In 8 fatal cases of accidental or intentional acute exposure of toluene, blood concentrations ranged from 10-48 mg/L (mean 22 mg/L). Interpretation of Urine Test Results: In 136 toluene abusers hospitalized or arrested while intoxicated, urine toluene concentrations ranged from 0-5 mg/L. Urinary o- - 86 - cresol and hippuric acid concentrations may have a high correlation with blood toluene concentrations. Hippuric acid excretion increases during the first 4 hours of exposure to up to 4 times the background level, then decreases rapidly to background levels within 6 hours. O-cresol excretion peaks during the last hour of chronic exposure or in the period immediately after acute exposure. Hippuric acid concentrations (not corrected for creatinine) in nonexposed persons averaged 800 mg/L (range 400-1400); daily exposure to 50 ppm averaged 1920 mg/L (range 1260-2930); 100 ppm ranged from 2800-3500 mg/L; and 200 ppm averaged 5970 mg/L (range 4120-8650). O-cresol is not normally detected in the urine of non-exposed persons, while exposure to 200 ppm results in concentrations of 1-3 mg/L. Effects: Psychological: Dizziness, euphoria, grandiosity, floating sensation, drowsiness, reduced ability to concentrate, slowed reaction time, distorted perception of time and distance, confusion, weakness, fatigue, memory loss, delusions, and hallucinations. Physiological: Irritation to the nose, throat, and eyes, headache, nystagmus, slurred speech, ataxia, staggering, impaired color vision, vigilance, nausea, vomiting, respiratory depression, convulsions, severe organ damage, coma, and death. Mild exposure (100-1500 ppm) dose-dependently results in euphoria, dizziness, reduced inhibitions, feelings of inebriation similar to alcohol intoxication, headache, nausea, lethargy, slow thought and speech, impairment of coordination, loss of memory, slowed reaction time, fatigue, sedation, confusion, impaired cognition function, impaired visual perception, staggering gait, muscular fatigue, and insomnia. More severe intoxication (10,000-30,000 ppm) will lead to tremors, arrhythmias, paralysis, unconsciousness, coma, and death. Chronic exposure may result in paranoid psychosis, temporal lobe epilepsy, mental retardation, and visual impairment. Side Effect Profile: Toluene can cause brain, liver and kidney damage, hearing loss, memory impairment, and attention deficits.

Discount gabapentin 600 mg fast delivery
Effects of capsicum fruit on theophylline absorption and bioavailability in rabbits. Effects of capsaicin on the pharmacokinetics of antipyrine, theophylline and quinine in rats. Capsicum + Theophylline Although capsicum may slightly increase the absorption of theophylline, it does not appear to be clinically relevant. Capsicum did not affect the pharmacokinetics of theophylline, apart from a 40% increase in the elimination rate constant after the single dose of capsicum. C Pharmacokinetics For information on the pharmacokinetics of an anthraquinone glycoside present in cascara, see under aloes, page 27. Interactions overview No interactions with cascara found; however, cascara (by virtue of its anthraquinone content) is expected to share some of the interactions of a number of other anthraquinonecontaining laxatives, such as aloes, page 27 and senna, page 349. Of particular relevance are the interactions with corticosteroids, digitalis glycosides and potassium-depleting diuretics. Constituents Anthraquinone glycosides are major components of cascara and include cascarosides A, B, C, D, E and F, aloins A and B, and chrysaloins A and B. Aloe-emodin, barbaloin, crysophanol, emodin, frangulin and physcion are also present in small amounts, as are resins and tannins. This serves as a reminder that in vitro studies cannot be directly extrapolated to the clinical situation, and that the findings need confirmation in a clinical setting. Note that there are two chemotypes of Uncaria tomentosa, one primarily containing the tetracyclic oxindole alkaloids, isorhynochophylline and rhynchopylline, and one primarily containing the pentacyclic oxindole alkaloids, (iso)pteropodine and (iso)mitraphylline. An in vitro evaluation of human cytochrome P450 3A4 inhibition be selected commercial herbal extracts and tinctures. In vitro inhibition of human cytochrome P450-mediated metabolism of marker substrates by natural products. In various preclinical studies, antiviral, anti-inflammatory, antirheumatic, immunostimulating, antimutagenic, antitumour and hypotensive properties have been shown. Importance and management Evidence appears to be limited to experimental data and an interaction is not established. Concurrent use need not be avoided, but patients should be made aware of the possibility of increased antihypertensive effects. Hypotensive and hemodynamic effects of isorhynchophylline in conscious rats and anaesthetised dogs. Warn patients to discuss any episode of prolonged bleeding with a healthcare professional. There were no safety concerns from the use of the combination when compared with placebo, and a modest clinical benefit. Randomized double blind trial of an extract from the pentacyclic alkaloid-chemotype of Uncaria tomentosa for the treatment of rheumatoid arthritis. Importance and management Evidence appears to be limited to one case report from which it is difficult to draw general conclusions. No evidence of protease inhibitor-related toxicity was found and the patient reported no adverse effects. The supplement was stopped and by day 15 the levels of all three drugs had returned to within normal limits. Not to be confused with celery stem, which is commonly eaten as a salad vegetable. Use and indications Celery seed is traditionally used for joint inflammation (including rheumatism), gout and urinary tract inflammation. C Pharmacokinetics No relevant pharmacokinetic data found for celery seed, but see flavonoids, page 186, and natural coumarins, page 297, for information on these constituents present in the herb. Other important constituents are the flavonoids (notably apigenin and isoquercitrin) and natural coumarins (bergapten, isoimperatorin, osthenol, umbelliferone and 8-hydroxy-5-methoxypsoralen), some of which may cause photosensitivity; however, celery seed oil has been reported to be non-phototoxic in humans. Note that celery stem contains much lower levels of the phototoxic natural coumarins; even so, cases of phototoxicity have been reported. For information on the interactions of individual flavonoids present in celery seed, see flavonoids, page 186. Although celery seed contains natural coumarins, the quantity of these constituents is not established, and therefore the propensity of celery seed to interact with other drugs because of their presence is unclear. Consider natural coumarins, page 297, for further discussion of the interactions of coumarin-containing herbs. Alkaloids of the pyridine type, including gentianine, gentianidine, gentioflavine, are also found in trace amounts.
Gabapentin 800 mg online
Further basic science experiments will help to elucidate other novel effects of the ketogenic diet. At the same time, a careful and systematic study of the clinical effects of the ketogenic diet in specific epilepsy syndromes with particular causes might provide useful clues regarding mechanisms of action (36). It is typical to see a transient hypoglycemia during the first few days, which does not require any treatment unless the child demonstrates symptoms. Treatment of asymptomatic hypoglycemia delays the metabolic adaptation of the child to the state of chronic ketosis. During the fast, the patient is offered water, sugar-free beverages, and unsweetened gelatin. This approach was compared to the traditional fasting implementation by Kim and colleagues. They found greater tolerability in the nonfasting group with no difference in time to ketosis or ultimate effectiveness of the diet at 3 months (38). In another study comparing fasting to nonfasting initiations, no difference was found in ultimate effectiveness of the diet, though the fasting group achieved ketosis more rapidly (39). If the child is fasted, then the urine usually reveals medium to large ketones after the 38-hour fast, and the diet is started. We never have children fast any longer than this, and a shorter period of fasting (24 hours) often suffices with infants and young children. Instead, the diet is begun at a reduced concentration on the first day of admission. It is computed to provide 75 to 100 kcal/kg body weight and 1 to 2 g of dietary protein/kg body weight per day. Caloric requirements are adjusted to minimize weight gain and to maximize ketonemia. If a 3:1 (fat-to-nonfat) ratio is insufficient to produce the required ketosis, then a ratio of 4:1 is used. Close observation is important, because children with certain underlying inborn errors of metabolism, particularly ones that interfere with the utilization of ketone bodies, could quickly decompensate (37). The hospitalization also provides the opportunity for family members to be instructed on the maintenance of the diet and the monitoring of blood -hydroxybutyrate concentrations. Urine ketones may be misleading and should not be monitored if blood measurements are available. The 3:1 ratio of the diet stipulates that 4 g of food must contain 3 g of fat and 1 g of nonfat. One gram of fat has the calorie equivalent of 9 calories, whereas 1 g of protein or carbohydrate has the calorie equivalent of approximately 4 calories. Four grams of food (arbitrarily referred to as 1 unit here) on a 3:1 diet is then equal to 31 calories: 1 g fat 9 calories 27 4 3 27 calories 1 4 calories 31 calories/unit 1 g protein and carbohydrate Total calories 4 calories To calculate the daily fat intake, one first divides the daily requirements of calories by this figure of 31 calories/unit, Chapter 69: the Ketogenic Diet 793 which generates the number of units required for the day: 1000 calories/day = 32. Thus far, the combination of 871 calories of fat and 80 calories of protein leaves only 49 calories (1000 951) not accounted for in the daily allowance. The carbohydrate intake is then calculated to supply the necessary remaining calories (49 calories), which in this case is approximately 12 g. A sudden stop of the diet or sudden administration of glucose may aggravate seizures and precipitate status epilepticus (41). Livingston advocated maintaining the diet at a ratio 4:1 for 2 years and, if successful, weaning down to a 3:1 diet for 6 months, followed by 6 months of a 2:1 diet (42). An example of this is pyruvate carboxylase deficiency, in which patients may present early in life with refractory myoclonic seizures (37). However, Kang and colleagues showed that the ketogenic diet may be used in selected circumstances, particularly in patients with respiratory chain defects (43). Patients with fatty acid oxidation problems would also be adversely affected by use of the ketogenic diet, but such patients do not, as a rule, present with seizures. The diet is contraindicated in patients with organic acidurias and porphyria (44).
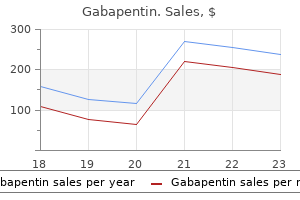
Real Experiences: Customer Reviews on Gabapentin
Altus, 63 years: The overall nationwide rate of graduation from high school is approximately 82%; for persons with epilepsy, this rate is approximately 64% (33). Anecdotally, some physicians have used plasma levels as an index of the ability of Chapter 56: Gabapentin and Pregabalin 16. The attenuation factor is defined by the inverse square law: That is, the recorded electrical potential falls off in direct proportion to the square of the distance from the generator (35,36).
Leon, 30 years: There are some medications that are designated as pill line only for certain indications (see page 12). If the compound is found to be promising, a drug company may decide to test it as a new drug on humans and it proceeds to the clinical trials stage. Patients should be monitored for signs and symptoms of psychiatric and behavioral adverse reactions including aggression, anger, irritability, hostility, and homicidal ideation and threats.
Hengley, 40 years: Effects of phenytoin and carbamazepine on cognitive functions in newly diagnosed epileptic patients. Varying degrees of white matter lesions may also be present along with cortical and cerebellar atrophy (80). Of course, the exact amplitude (in absolute terms) at any scalp electrode is unknown.
Temmy, 46 years: For example, a recent study found that the average neurology outpatient visit for epilepsy in the community setting lasted 12 minutes (1). Spreading in itself would not be an insurmountable problem, because it is theoretically possible to recover deep dipole sources based on observed surface potentials, using appropriate mathematical transformations. Use of dietary supplements and their interactions with prescription drugs in the elderly.
Amul, 24 years: It does mean you work together with your health care team, family, and other supports. The incidence of catamenial epilepsy varies from 10% to 78% in studies due to the different criteria used by investigators to meet the term catamenial epilepsy. Monotherapy of Monotherapy Few clinical trials have evaluated the use of zonisamide in monotherapy for the treatment of epilepsy.
10 of 10 - Review by Z. Ur-Gosh
Votes: 82 votes
Total customer reviews: 82
References
- Borda E, Agostini M, Gimeno MF, et al: Alpha and beta sympathetic responses to isoproterenol by the isolated rat vas deferens, Pharmacol Res Comm 13:487n499, 1981.
- Steiner H, Bergmeister M, Verdorfer I, et al: Early results of bladder-cancer screening in a high-risk population of heavy smokers, BJU Int 102:291-296, 2008.
- Crisci KL, Greenberg SB, Wolfson BJ. Cardiopulmonary and thoracic tumors of childhood. Radiol Clin North Am 1997;35:1341-66.
- Reisiger K, Landman J, et al: Laparoscopic renal surgery and the risk of rhabdomyolysis: diagnosis and treatment, Urology 66(5 Suppl):29-35, 2005.
- Ell C, May A, Pech O, et al: Curative endoscopic resection of early esophageal adenocarcinomas (Barrett's cancer). Gastrointest Endosc 65:3, 2007.
- Washburn KK, Zappitelli M, Arikan AA, et al. Urinary interleukin- 18 is an acute kidney injury biomarker in critically ill children. Nephrol Dial Transplant. 2008;23:566-572.