
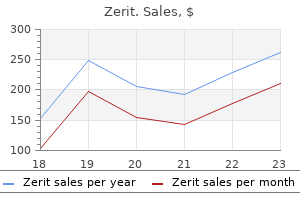
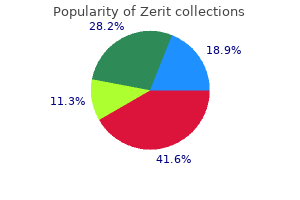
Zerit dosages: 40 mg
Zerit packs: 30 pills, 60 pills, 90 pills

Discount zerit 40 mg overnight delivery
With persistent contraction of the anal sphincter from rectal stool impaction, the pelvic flooring musculature equally contracts inappropriately, leading to secondary detrusor�external urinary sphincter dyssynergia. Limiting free entry to a restroom or, worse, discouraging voiding in response to urgency in a child who has not developed full cortical inhibition of voiding may alter normal coordination between bladder and sphincter (McKenna and Herndon, 2000). Between 20% and 40% of youngsters with daytime urinary incontinence are affected by comorbid behavioral issues (von Gontard et al, 1998b; Joinson et al, 2006). This is 2 to 4 instances higher than kids with out enuresis and is comparable with charges of psychosocial problems in different pediatric continual sickness groups. Other studies have investigated the psychological problems associated with particular syndromes answerable for daytime urinary incontinence. These investigators discovered a better price of conduct issues in children with voiding postponement in comparison with these with urge incontinence as their main grievance (Lettgen et al, 2002; von Gontard et al, 2011a). Moreover, some have instructed that voluntary holding with postponement of voiding is acquired and may be reflective of ongoing behavioral points (von Gontard et al, 1999). Of the 358 patients examined, 32% had a recent life stressor and 23% had a comorbid psychiatric disorder. In maybe one of the largest epidemiologic studies to have a look at the affiliation between daytime urinary incontinence and neuropsychiatric issues in youngsters, researchers found a significantly increased rate of psychological problems amongst youngsters who wet themselves compared to those that were dry (Joinson et al, 2006). In a secondary analysis, they also sought to decide if constipation and encopresis, which are sometimes presumed to coexist, also coexisted for his or her specific cohort. The majority of sufferers with encopresis with or without related constipation had idiopathic detrusor overactivity, and people with the worst urgency were those reporting encopresis. Interestingly, in kids with encopresis, severe urgency was generally reported and after initiation of anticholinergic therapy the encopresis incessantly resolved even earlier than the urgency had absolutely subsided. Clearly, there continues to be a void in our understanding of the bowel and bladder interplay in higher cortical facilities and the spinal cord. Moreover, this fostered uncertainty and made it quite troublesome to evaluate analysis and study outcomes amongst totally different teams. The diary should embody voided volumes, timing of each void and incontinent episode, timing of every bowel motion and fecal soiling episode, and fluid consumption. Urine loss is quantified by recording if clothing had to be modified after the urine loss (significant urine loss) or not. The 10 questions were assigned scores of zero to three according to incidence within the month earlier than responding to the questionnaire and responses are weighted equally, giving a most possible score of 30. The targets of analysis are firstly to determine whether the affected person has a filling or emptying (or both) section abnormality. If an abnormality is discovered, the evaluation should then be directed toward figuring out the underlying cause and distinguishing whether the dysfunction stems from an anatomic or practical concern. This final point is crucial as a end result of the management technique will depend on the cause. It consists of 20 questions associated to urinary incontinence high quality of life that are graded on a scale of zero to 4 (0 = No, 1 = Hardly ever, 2 = Sometimes, three = Often, four = All the time) with a complete attainable rating of eighty. The preschool guidelines accommodates one hundred questions and the school-age checklist contains a hundred and twenty questions, with responses recorded on a Likert scale. PhysicalExamination the physical examination is targeted on genitourinary anatomy and neurologic perform. For occasion, yellow stains in the underwear may be an indicator of urge or overflow incontinence or postvoid dribbling. In a toddler with constipation, the abdominal examination might detect tenderness of the left higher and decrease quadrants resulting from colonic distention secondary to fecal impaction and/or gaseous distention. The concept is that elevated bladder pressures can result in retrograde reflux of caustic urine into the ejaculatory ducts, resulting in inflammation alongside the course of the vas deferens, epididymis, and testes. These embrace an asymmetrical gluteal cleft, a presacral dimple, a lipoma, a hair tuft, a dermal sinus tract, and a dermal vascular malformation. Examination of the labia and vaginal introitus is carried out to detect any proof of labial adhesions. Areas of skin excoriation or redness may be present and are often a sign of steady or extreme urinary leakage with persistent inflammation and less often secondary to fungal infection. Neurologic Examination A targeted neurologic examination ought to include assessing lower extremity strength and deep tendon reflexes, gait, perineal and anal sensation, and rectal tone. The child voids into a set device that produces a urinary flow curve providing the utmost (Qmax) and average (Qavg) urinary flow charges, voided quantity, move time, and shape of urine circulate.
Order 40mg zerit mastercard
We have used transurethral injection of collagen and dextranomer around the bladder neck to enhance outlet resistance and stimulate the bladder to develop. However, in our hands this has not been as successful as reported by Caione and colleagues (1993a, 1993b). If the bladder neck or urethra or both are problematic, a catheterizable continent stoma with or without bladder neck plasty or transection is carried out, together with augmentation (Gearhart et al, 1995b). FailedBladderNeckRepair Even with skilled exstrophy surgeons, missteps can occur, and there remains a subgroup of children with urinary incontinence after bladder neck reconstruction secondary to (1) insufficient outlet resistance; (2) a small bladder capability (lack of progress after bladder neck reconstruction); (3) decreased compliance; or (4) a mixture of those factors. In these situations urethral bulking agents have been used in an try and avoid additional major reconstructive procedures (Burki et al, 2006). Formerly, collagen was the bulking agent of choice, but often multiple injections have been required (Ben-Chaim et al, 1995a). In a large sequence from Paris, Lottmann and colleagues (2006) reported on the utilization of a dextranomer-based bulking agent in childhood with incontinence from a number of causes. Of the 9 exstrophy patients, 4 achieved success; in the epispadias group the success fee was a lot higher (longer than 3 hours dry by intermittent catheterization or voiding). In a current very massive series of particularly exstrophy-epispadias patients (Shah et al, 2014) with a median follow-up of eight years, 41 underwent injection earlier than bladder neck reconstruction and 25 after bladder neck reconstruction. This has been reported in as few as 4% and as many as 19% of instances (Kajbafzadeh et al, 1995; Surer et al, 2000). Urethral tortuosity with difficult catheterization or strictures are unusual with modern epispadias repair. Since the applying of the penile disassembly for epispadias reconstruction, newer, more vital problems have been famous (Hammouda, 2003). Gearhart and Baird (2005) have reported lack of the glans, corpora, or both along with loss of penile skin and the urethral plate. Whether that is secondary to surgical misadventure, vagaries within the blood provide of the penis, or the intrinsic difficulties within the procedure remains a subject of debate. Reconstruction of these complications has required extra methods including tissue growth, full-thickness pores and skin grafting, buccal mucosal grafting, and other advanced strategies. In some patients with significant losses, neophalloplasty might finally present the fabric for final beauty reconstruction. This different allows a sensate beauty neophallus for this particular group of exstrophy failures. At an older age, unsightly penile scars and a brief phallus could prompt further surgical intervention. Scar excision could be closed in a plastic style if sufficient penile pores and skin is available. In extreme instances, tissue expanders could be positioned beneath the penile pores and skin and gradually inflated over 6 weeks to enable extra penile pores and skin and obviate the necessity for grafting. Freeing all scar tissues and suspensory ligament tissue can maximize available penile length. A dorsal dermal corporeal graft or ventral corporeal plication or rotation may also help lengthen as well as correct any chordee. Therefore, overly aggressive makes an attempt at penile lengthening could result only in corporeal denervation and devascularization without further lengthening. Chapter139 Exstrophy-EpispadiasComplex 3217 exstrophy-epispadias complicated who confirmed wonderful continence charges with long-term higher tract preservation compared with standard ureterosigmoidostomy. Their suggestion for treatment in a selection of patients with severely impaired renal function was that a colonic conduit was the most effective method of choice for diversion. In the sufferers with a traditional or slightly dilated upper tract and intact anal sphincters, a Mainz rectal reservoir was really helpful. Although the group from Mainz reported no most cancers in a long-term follow-up study of sufferers who underwent ureterosigmoidostomy, the danger for malignancy still exists. All patients with a ureterosigmoidostomy ought to have a yearly renal ultrasound and colonoscopy in grownup life. Additional causes for looking for different methods of remedy embrace failure of preliminary closure with a small remaining bladder or failure of continence surgery, or both. This protects the kidneys from vesicoureteral reflux, and undiversion could be carried out when clinically indicated at an older age.
Order zerit 40 mg with visa
A 6-Fr to 12-Fr stent is usually left for 10 to 14 days throughout the efferent catheterizable channel through the healing course of. It is then advisable for the surgeon to personally catheterize the efferent limb earlier than the affected person or members of the family do so. Catheterization ought to be repeated a minimal of each 4 hours during the day for reservoir drainage, upkeep of patency, and minimalization of the chance of stomal stenosis. The appendix is in all probability not obtainable for use in all patients owing to previous appendectomy, its location or size, congenital absence, involvement with adhesions, or its use for continence enemas. Histologic abnormalities of the appendix have been reported to occur in as many as 30% of sufferers (Liebovitch et al, 1992) and to enhance with age. They rarely are of enough scientific significance to preclude use (Mulvihill et al, 1983). Several papers have reviewed large sequence of patients after appendicovesicostomy (Kaefer et al, 1997b; Cain et al, 1999; Harris et al, 2000; Thomas et al, 2006; Welk et al, 2008; VanderBrink et al, 2011). Inability to use the appendix, apart from as a end result of it was needed for use in situ for antegrade continence enemas, has been rare. The outcomes, by method of continence, have been excellent, normally above 95% (Kaefer and Retik, 1997; Mor et al, 1997; Suzer et al, 1997; Gerharz et al, 1998; Gosalbez et al, 1998; Cain et al, 1999; Castellan et al, 1999; Liard et al, 2001; Elshal et al, 2011; VanderBrink et al, 2011; Baradaran et al, 2012). Incontinence is a rare occasion with the Mitrofanoff precept and will outcome from inadequate size of the flap valve mechanism or persistently elevated reservoir stress. Injection of a bulking agent is a attainable treatment for insufficient outflow resistance, with success reported up to 50% in the quick term (Welk et al, 2008). A more formal approach with takedown and revision of the leaking Mitrofanoff valve is usually required (Kaefer and Retik, 1997) the commonest complication has been stomal stenosis, which in general has occurred in 6% to 10% of patients (Thomas et al, 2006; Welk et al, 2008; Leslie et al, 2011; Ardelt et al, 2012). Stenosis leading to troublesome catheterization might happen early in the postoperative course and require formal revision (Harris et al, 2000). Mickelson and coworkers (2009) have described the successful use of an "L stent" with topical steroid cream as an efficient noninvasive treatment. Most problems with stomal stenosis and creation of a false passage (perforation) happen within the first few years after reconstruction, however long-term problems do happen, ensuing in the want for lifelong monitoring (Thomas et al, 2006; Leslie et al, 2011). Benign fibroepithelial polyps and inflammatory granulomatous tissue have just lately been reported in all forms of catheterizable channels. Groth and associates (2013) reported an incidence of polyps occurring in 20% of their sufferers at a 7-year follow-up, with 50% being symptomatic and 45% having a recurrence after resection. Stricture and necrosis, notably of cecal extensions of the appendix, have occurred rarely. Abdominal stomas may be associated with a better risk of reservoir calculi owing to the potential for incomplete emptying. Similar outcomes have been achieved in smaller series of adults (Gowda et al, 2008; Van der Aa et al, 2009; Ardelt et al, 2012). When the appendix is unavailable for use, other tubular structures can provide an identical mechanism for catheterization and continence. Mitrofanoff (1980) described an identical method utilizing ureter (Kaefer et al, 1997b). Refluxing ureters have even been used after extravesical reimplantation (Ashcraft and Dennis, 1986; Duel et al, 1996; Kaefer et al, 1997b). Stomal stenosis seems to be more problematic with use of the ureter compared with the appendix, possibly due to compromised blood supply. In addition, distention of the ureter from catheter passage has brought on discomfort in some individuals (Duckett and Lofti, 1993). Woodhouse and MacNeily (1994) used the fallopian tube, which may accommodate catheterization. Ileum has been tapered to create a similar uniform tube of sufficient length (Adams et al, 1992). By narrowing the ileal section longitudinally alongside the mesenteric border utilizing permanent staplers in sequence, a surrogate was constructed that was straightforward to catheterize and provided good continence. Others (Woodhouse and MacNeily, 1994; Hampel et al, 1995) have shown comparable success with tapered ileum. The catheterizable channel have to be long sufficient to attain from the reservoir to skin without rigidity, but stored as brief and straight as potential to facilitate straightforward catheterization. An unnecessarily lengthy, cell catheterizable channel can kink and end in troublesome catheterization or perforation. Yang and Monti have been credited with a novel modification of the tapered intestinal segment that can be reimplanted based on the Mitrofanoff principle (Yang, 1993; Monti et al, 1997).
Generic zerit 40mg otc
It appears that repeated injections proceed to be effective, with the interval between repeated injections rising with every sequence of injections (Schulte-Baukloh et al, 2005; Altaweel et al, 2006). Repeated injections have been related to a major lower within the quantity of fibrosis compared with those with no history of injection (Pascali et al, 2011). Although some studies have proven improvement in clinical and urodynamic parameters, larger, prospective, randomized trials are required (Godec and Cass, 1978; Decter et al, 1992, 1994; Balcom et al, 1997; Marshall and Boston, 1997; Han et al, 2004; Cirovi et al, 2009; Kajbafzadeh et al, 2009, 2010; Choi et al, 2013a). Sacral Neuromodulation Sacral neuromodulation has been used extensively in youngsters with non-neurogenic bladder dysfunction. Seven % of the neuromodulation group required revision surgical procedure (Guys et al, 2004). Thus, sacral neuromodulation on this population appears to be protected with some limited advantages over normal remedy, however a larger examine is required to decide its efficacy. Presenting signs embrace abdominal distention and pain, septic shock, and shoulder ache related to diaphragmatic irritation from extravasated urine (Bauer et al, 1992). Sepsis resulted in demise in 25% of patients with bladder perforation in a single series (Bauer et al, 1992). Those with a history of bladder outlet procedures seem to be at elevated threat (Bauer et al, 1992; Metcalfe et al, 2006b). It seems that these with a catheterizable belly stoma are at decrease risk of perforation (Metcalfe et al, 2006b), perhaps due to elevated compliance with catheterization schedules (Horowitz et al, 1995). Because of the danger of sepsis and demise, analysis and therapy must be immediate. It is postulated that overdistention and relative ischemia associated to bowel detubularization are necessary within the pathophysiology of rupture (Bauer et al, 1992). The gold normal strategy to management of this drawback is exploratory laparotomy and closure of the perforation; nevertheless, conservative administration with drainage of the urinary reservoir and percutaneous drainage of abdominal urinoma in sufferers without hemodynamic instability or worsening signs has been described (Slaton and Kropp, 1994; Leyland and Masters, 2003). Augmentation cystoplasty with any segment of the gastrointestinal tract can result in long-term consequences in acid-base stability, vitamin B12 deficiency, fats absorption, renal function modifications, aberrant bone metabolism, and progress retardation (Gilbert and Hensle, 2005). Early reviews instructed that intestinal and gastric bladder augmentation were related to an elevated threat of bladder cancer. Most research note a 10-year minimal lag time between the augmentation and presentation of illness. Age at presentation is younger than is typical for bladder most cancers (Austin et al, 2007; Veenboer and Kort, 2011). One examine found that just about 90% of patients had regionally advanced illness or lymph node metastases at presentation (Austin et al, 2007). Urothelial cell carcinoma accounts for near 60% of the tumors, adopted by squamous cell carcinoma in 21%, adenocarcinoma in 16%, and signet cell tumor of the gastric increase in 5% (Austin et al, 2007). Some studies have disputed the association of enteric augmentation and an elevated danger of malignancy. For example, there have also been reviews of malignancy in these with autoaugmentation with out incorporation of enteric segments (Mehan et al, 2011; Veenboer and Kort, 2011). Sigmoid, cecum, stomach, and small intestine have been used to enlarge the bladder. Detubularization of the bowel is needed to minimize the intrinsic contractions of the intestinal section and prevent it from causing intractable incontinence as quickly as it has been added to the bladder (Goldwasser et al, 1987; Hinman, 1988). Most studies evaluating outcomes for augmentation cystoplasty have patient populations with mixed causes (primarily neurogenic bladder but in addition other etiologies such as exstrophy-epispadias, posterior urethral valves, and so on), and augmentation cystoplasty is carried out with and without concomitant procedures such as continent catheterizable channels, antireflux surgical procedure, and bladder outlet procedures. Thus there are limited data that mirror the outcomes specifically in those with neurogenic bladder handled with augmentation cystoplasty in isolation. Continence is achieved in 90% or extra (Shekarriz et al, 2000; Husmann and Cain, 2001; Quek and Ginsberg, 2003; Veenboer et al, 2013). Increased imply bladder capacity (Krishna et al, 1995; Quek and Ginsberg, 2003), improved compliance (Veenboer et al, 2013), and safe storage pressures (Krishna et al, 1995; Quek and Ginsberg, 2003) are achieved in most patients. Postoperative urodynamic research might reveal common phasic contractions (Robertson et al, 1991). It is unclear if these contractions come up from the bowel section or the remaining bladder. These contractions are normally of low-amplitude activity (<40 cm H2O), and are volume dependent, occurring only at volumes above 200 mL (Quek and Ginsberg, 2003). Zero to 29% of sufferers require antimuscarinics after augmentation (Mitchell et al, 1986; Luangkhot et al, 1991; Herschorn and Hewitt, 1998; Chartier-Kastler et al, 2000; Quek and Ginsberg, 2003). The complication fee of augmentation cystoplasty is roughly 30% (Metcalfe et al, 2006b; Schlomer et al, 2013).

Order zerit 40mg on line
Microscopically, the cysts are lined by low cuboidal epithelium, are surrounded by collars of spindle cells, and are full of proteinaceous or sanguineous fluid. They are separated by skinny septa of fibrous tissue and primitive dysplastic components, particularly primitive ducts. Frequently, immature glomeruli are present, and once in a while a couple of mature glomeruli are seen. Intervention for these massive plenty could need to be undertaken to relieve these issues. The likelihood of malignant transformation is estimated to be extremely low and believed by many to be nonexistent (Avni et al, 1987; Gordon et al, 1988; Wacksman and Phipps, 1993; Narchi, 2005b). Many pediatric urologists will perform ultrasound surveillance every three to 12 months, however there has been no conclusive evidence that this is useful or cost-effective (Perez et al, 1998; Onal and Kogan, 2006). The numerous case reports and small sequence that have been reviewed provide conflicting data on the problem. There has been some debate as to whether or not these lesions characterize a spectrum of 1 illness with a standard trigger. However, controversy continues about whether or not the multilocular cyst is a segmental form of renal dysplasia (Powell et al, 1951, Osathanondh and Potter, 1964; Johnson et al, 1973), a hamartomatous malformation (Arey, 1959), or a neoplastic disease (Boggs and Kimmelsteil, 1956; Christ, 1968; Fowler, 1971; Gallo and Penchansky, 1977). The confusion arises in part from the variability of the histologic image: the appearance of the primitive stroma; the maturity of tubular and even on occasion of muscle parts; and the degree of epithelial atypia that differs not solely from affected person to patient but also within the similar lesion. Treatment the treatment for any multilocular cystic lesion, even the most benign variant, is nephrectomy. In adults, benign multilocular cysts more usually are related to bigger amounts of normal renal tissue, making partial nephrectomy more typically possible. By comparability, if a clear cell sarcoma is found after enucleation, the remaining ipsilateral renal tissue should be eliminated because of the aggressiveness of this most cancers. The recurrence of a multilocular cyst not containing malignancy in all probability reflects insufficient excision of the preliminary lesion. ClinicalFeatures the nice majority of cases (95%) manifest before the age of four years or after 30 years. If youthful than four years, the affected person is twice as likely to be male; if older than 30 years, the affected person is eight times as likely to be feminine (Eble and Bonsib, 1998). In children, an asymptomatic flank mass is the most common discovering, whereas most adults have a flank mass, belly pain, or hematuria. The bleeding is felt to be secondary to herniation of the cyst by way of the transitional epithelium into the renal pelvis (Uson and Melicow, 1963; Aterman et al, 1973; Madewell et al, 1983). Seven cases of bilateral benign multilocular cysts of the kidney have been described (Castillo et al, 1991), and recurrence after excision has been hardly ever described (Geller et al, 1979). There are additionally a minimum of two cases during which multilocular cysts arose in kidneys recognized to have been normal beforehand (Uson and Melicow, 1963; Chatten and Bishop, 1977). The lesion could prolong beyond the renal capsule into the perinephric space or renal pelvis. They contain clear, straw-colored or yellow fluid and are lined by cuboidal or low columnar epithelial cells. In some cases, eosinophilic cuboidal cells project into the cyst lumen, making a hobnail appearance (Madewell et al, 1983). In youngsters, though there could also be a continuum from benign multilocular cyst to cystic Wilms tumor, and although all of those lesions may be derived from related cells or tissues, no proof suggests that one entity transforms into another. Furthermore, none of the genetically determined situations related to Wilms tumor. The cystic component of the tumor on the carcinomatosis end of the spectrum in each children and adults. They are often oval to spherical; may be solitary or multiple, unilateral or bilateral; and are filled with plasma-like clear or straw-colored fluid (Nahm and Ritz, 2000; Terada et al, 2002). Simple cysts could manifest at any time in utero and have been identified as early as 14 weeks of gestation. However, in adults the frequency rises with age, with an incidence of 20% by age 40 years and as excessive as 50% after age 60 years (Kissane and Smith, 1975; Laucks and McLachlan, 1981). Most stories present no gender predilection; nevertheless, in a minimum of two research, men were affected more incessantly than ladies (Bearth and Steg, 1977; Tada et al, 1983).
Papaw (Papaya). Zerit.
- Dosing considerations for Papaya.
- Stomach and intestine problems, parasite infections, and other conditions.
- Are there safety concerns?
- How does Papaya work?
- Are there any interactions with medications?
- What is Papaya?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96494
Generic zerit 40mg line
When an infant survives-because the obstruction is incomplete or as a outcome of there was decompression owing to an antenatal shunt placement or a patent urachus-the end result can be similar to that of a child with obstructing posterior urethral valves (Gonz�lez et al, 2001). An obstructing membrane is typically seen on the distal end of the prostatic urethra and the urethra distal to that time could additionally be hypoplastic. Since the condition is often found in association with a large anterior urethral diverticulum, the valve itself is varyingly described as an obstruction resulting from a wall of the diverticulum obstructing flow or a semilunar fold draping down from the wall of the anterior urethra and interrupting urinary flow (Tank, 1987; Paulhac et al, 2003). A rupture of dilated bulbourethral glands has additionally been instructed as an etiology (McLellan et al, 2004). The valves may be positioned at the bulbar urethra, the penoscrotal junction, or the penile urethra (Firlit et al, 1978). Patients current with anterior urethral valves at different ages based mostly on the severity of the obstructive process. Symptoms could encompass postvoid dribbling and mild incontinence, vital bulging of the distal penis, palpable bladder with obstruction or even renal insufficiency, and urinary tract infections (Cruz-Diaz et al, 2013). Diagnosis requires a careful examination of the external genitalia, and compression of the distal shaft might end in expressing of urine as seen in a diverticulum. A voiding cystourethrogram is required to verify the analysis and will demonstrate a dilated anterior urethra with proximal indicators of continual obstruction, together with bladder diverticula and big vesicoureteral reflux. Cystoscopic image on the second day of life in a neonate with a prenatal historical past of decrease urinary tract obstruction. UrethralDuplication Urethral duplication is another rare anomaly of the urethra with a quantity of recognized anatomic variants. Whereas one urethra often terminates on the glans close to its orthotopic place, another urethra may finish in a meatus placed on the glans or extra ventrally alongside the shaft of the penis. In the most extreme cases, the duplicated urethra may even be as proximal as the anal sphincter. The duplication happens in a sagittal aircraft, with the ventral urethra normally the useful meatus containing the sphincteric advanced and verumontanum. Effmann and associates (1976) are credited with the most extensively used classification system for urethral duplications. Broadly, the sort I abnormality includes a blind incomplete urethral duplication or accessory urethra. Diagnosis is instantly made in some instances when two distinct meatal openings are seen on the glans, but in other instances requires a high index of suspicion when inspecting what appears to be an atypical case of proximal hypospadias with a patent-appearing opening on the glans. A voiding cystourethrogram will affirm the diagnosis during the voiding phase in lots of circumstances, although a retrograde injection of the distinct urethra may also be accomplished. Surgical administration is complicated and should require a selection of single or multiple-stage repairs. Whereas the small, blind-ending accent urethra could additionally be handled expeditiously with simple coagulation of the mucosal tract with a Bugbee electrode, a patent duplicated urethra related to the bladder with a definite bladder neck will require a planned reconstruction. Alanee and colleagues (2012) recently described a way by which the septum between the two urethral channels is incised and the dorsal defect is repaired with reverse glans wings to cowl a dorsal urethroplasty. In instances in which the urethral openings are separated by the Y-type association, a staged reconstruction utilizing preputial or buccal mucosa flaps is usually required to deliver the extra ventral, however practical, meatus to the glans penis the place it can be insinuated into the dorsal, often atretic, urethra. Urethrorrhagia Urethrorrhagia, usually referred to as idiopathic urethrorrhagia, describes a spotting of blood on the underwear after urination, or voiding of clear urine adopted by a quantity of drops of blood. The seen blood tends to elevate alarm inside households, however the condition is often thought-about benign and self-limited. The etiology of urethrorrhagia is unclear, though numerous hypotheses have been offered. Meatal stenosis and dysfunctional elimination syndrome have been suggested as inciting factors (Herz et al, 2005). Proponents of voiding dysfunction because the etiology of urethrorrhagia maintain that elevated voiding pressures attributable to incomplete leisure of the exterior urethral sphincter lead to turbulent flow that creates a adverse intraluminal urethral stress. That unfavorable stress causes an engorgement of the sinuses of the urethral mucosa and a small extravasation of blood (Docimo et al, 1998; Herz et al, 2005). Rather, evaluation ought to focus on a detailed history of bowel and bladder perform, renal and bladder ultrasonography, and an workplace analysis of urinary flow rate and postvoid residual. If urethrorrhagia becomes atypical-accompanied by symptoms of urethral stricture or increased urethral bleeding- then cystoscopy must be carried out. Although the overwhelming majority of cases of urethrorrhagia will have an idiopathic origin, urethral strictures are identified throughout evaluation in 14% to 60% of sufferers (Dewan and Wilson, 1996; Poch et al, 2007).
Syndromes
- Foreign objects in the ear
- Your pregnancy is harmful to your health (therapeutic abortion).
- Using a soft-bristle toothbrush
- Weight gain (unintentional)
- Your hair does not improve with gentle treatment
- Nuclear heart scan (MUGA, RNV)
- Loss of alertness (unconsciousness)
Discount generic zerit canada
Once a volcano appearance with the ureteral meatus on high of the mound is achieved, additional quantity is injected till the ureteric orifice becomes crescent or slit shaped. The form of the achieved mound was discovered to be a major predictor of a successful consequence. Achieving a volcanoshaped mound was related to an 87% success fee, whereas different morphologies had been related to solely a 53% successful price (Lavelle et al, 2005). For most supplies, the needle should be stored in place for 1 minute at the end of the injection to scale back extrusion of the material on the injection web site. The bladder is emptied, and the mound is inspected with an empty and a full bladder to be sure that enough help of the ureter is persistent. This is best dealt with by emptying the bladder and applying gentle stress with the tip of the scope until the bleeding stops. In common the child spends a short period of time in the restoration room, adopted by discharge. In a examine by Herz and colleagues (2001) the importance of the training curve was highlighted. In the primary 6 months of their study the success price was 46% in 18 youngsters with 28 refluxing ureters. In the remaining 18 months of that research, the general correction rate was 93% in fifty six children with eighty four refluxing ureters after a single endoscopic injection. Although the approach is type of simple as soon as discovered, there are some technical nuances and particulars that require particular attention. If reflux is persistent, a repeat injection can be thought of 6 months after the preliminary injection. At open surgery the injected material is both not seen in any respect or is found properly encapsulated but in an incorrect airplane or location inside or outside the bladder. The material is well eliminated en bloc, and the open reimplant process carried out without problem. It ought to trigger minimal local irritation, whereas at the same time be well encapsulated by normal fibrous tissue and fibrocytes. The material must be easy to inject via a protracted needle that passes simply via most standard endoscopic devices. It should be viscous sufficient to stop leakage from the puncture site and preserve its injected volume and the mound form after the normal strategy of exchange and excretion of any carrier molecules. These materials can be categorised as particulate or degradable and autologous or nonautologous (Box 137-1). The concern with the particulate brokers is migration and with degradable brokers is sturdiness. The first is growth of the injected bolus, which may result in disruption of the small vessels in the space of the distal ureter and trigone, resulting within the material gaining intravascular entry. Particles smaller than 50 �m could bypass the pulmonary vascular mattress and thus entry the systemic circulation and reach different organs in the body. The second migration mechanism is by phagocytosis of the injected particles by tissue macrophages or blood-borne monocytes. It has been used for the manufacturing of vascular grafts, cardiac valves/implants, surgical sutures, cosmetic surgical procedure, and patches for hernia repairs (Monaghan and Meban, 1991; Godin et al, 1995; Sayers et al, 1998; Briguori et al, 2001). Teflon paste additionally was used as an injectable agent for embolization of vessels (Weingarten and Kauffman, 1977), for injection of vocal chords (Kasperbauer, 1995), and as a bulking agent for urinary incontinence (Politano, 1992). Matouschek (1981) first reported on the utilization of Teflon paste as a bulking agent for correction of reflux. A large European multicenter survey reported on 6216 ureters and 4166 youngsters with 10 years of follow-up and demonstrated a cure rate of 86% after one to four injections (Puri et al, 1995). The longest follow-up is out there from Dublin; 247 patients treated with Teflon paste with eleven to 17 years of follow-up demonstrated a sustained success rate of 95% with a 5% recurrence price (Chertin and Puri, 2002). Malizia demonstrated in experimental research that the particles can migrate to regional lymph nodes and to distant organs, including the lung and the mind (Malizia et al, 1984a, 1984b). Particle migration is believed to be related to the small size of the Teflon paste particles, which range from 4 to a hundred �m, with 90% of the particles lower than forty �m.
Purchase 40mg zerit otc
A single-centre long-term end result analysis of synthetic urinary sphincter placement in children. Long-term evaluation of metabolic profile and bone mineral density after ileocystoplasty in youngsters. Colocecal bladder augmentation with a tapered continent ileal limb: use in the neuropathic bladder. Pathogenesis of nocturnal urinary incontinence after ileocecal bladder alternative: steady measurement of urethral closure strain during sleep. The Pippi Salle process for neurogenic urinary incontinence in childhood: a three-year experience. Concomitant bladder neck closure and Mitrofanoff diversion for the management of intractable urinary incontinence. The impact of medium-fill and slow-fill saline cystometry on compliance and detrusor pressure in infants and kids with myelodysplasia. Presented at: Evidence-Based Practice in Spina Bifida: Developing a Research Agenda assembly. Autologous cell-seeded biodegradable scaffold for augmentation cystoplasty: part 2 examine in youngsters and adolescents with spina bifida. Does the kind of bladder augmentation affect the resolution of pre-existing vesicoureteral reflux Effects of the artificial urinary sphincter on prostatic improvement and sexual operate in pubertal boys with meningomyelocele. Prerequisite for profitable surgical outcome in urothelium lined seromuscular enterocystoplasty. Upsizing of the synthetic urinary sphincter cuff to facilitate spontaneous voiding. Teapot ureterocystoplasty and ureteral Mitrofanoff channel for bilateral megaureters: technical factors and surgical results of neurogenic bladder. Fascial sling for the management of urinary incontinence as a result of sphincter incompetence. Same setting laparoscopic antegrade continence enema and antegrade bladder neck injection for constipation and urinary incontinence within the spina bifida inhabitants. Appendicovesicostomy: a helpful adjunct to continent reconstruction of the bladder. Lyophilized human dura as a bladder wall substitute: experimental and medical outcomes. Chronic renal failure and bladder augmentation: stomach versus sigmoid colon within the canine model. Severe bladder trabeculation obviates the necessity for bladder outlet procedures during augmentation cystoplasty in incontinent patients with neurogenic bladder. Complications after bladder augmentation or substitution in youngsters: a potential examine in 86 sufferers. Incontinence following bladder neck reconstruction-is there a job for endoscopic administration Calcification of glutaraldehyde cross-linked collagen in bladder neck injections in kids with incontinence: a long-term complication. Bony demineralization following ureterosigmoid anastomosis: an experimental research in rats. Internal "reservoir" in sufferers with permanent ileostomy: preliminary observations on a process leading to fecal "continence" in five ileostomy sufferers. Urinary diversion to the augmented and valved rectum: preliminary outcomes with a novel surgical procedure. Clinical and urodynamic features of a brand new intestinal urinary sphincter for continent urinary diversion. Long-term followup and time to event end result evaluation of continent catheterizable channels. Non-traditional management of the neurogenic bladder: tissue engineering and neuromodulation. The frequency of histopathological abnormalities in incidental appendectomy in urological sufferers: the implications for incorporation of the appendix in urinary tract reconstruction. Reconstruction of the decrease urinary tract: observations on bowel dynamics and the synthetic urinary sphincter. Combined use of bowel and the bogus urinary sphincter in reconstruction of the lower urinary tract: infectious complications. Alteration in detrusor behavior and the impact on renal function following insertion of the artificial urinary sphincter.
Purchase zerit toronto
Conceptually that is efficient; nonetheless, issue with catheterization is a standard downside and significant concern. It is now recognized that occlusion of the bladder neck in children with neurogenic sphincter incompetence can end result in the unmasking or improvement of detrusor hostility manifesting with a decrease in bladder compliance or increase in detrusor overactivity (Bauer et al, 1986; Bauer, 2008). When hostile bladder characteristics are discovered preoperatively, anticholinergic medications could be useful for hyperreflexic contractions, however augmentation cystoplasty is usually required for diminished compliance. Light and colleagues (1995) reported a 50% infection fee with simultaneous augmentation in contrast with 9. To the opposite, a contemporary evaluation by Miller and coworkers (1998) found an infection necessitating elimination of the device occurred in only 2 of 29 such sufferers (7%). This low price is similar to that famous by others (Gonzalez et al, 1989b; Strawbridge et al, 1989). Several stories have evaluated varied components and located that the intestinal section chosen for augmentation appeared to be the only parameter affecting results; gastric augmentation was the least offensive regarding infection (Ganesan et al, 1993; Miller et al, 1998; Holmes et al, 2001). They achieved continence in 89% without the need for additional procedures and with no deterioration of the higher urinary tract. The cuff supplies static, fixed resistance that enhances continence and permits for intermittent catheterization. The injection port is positioned subcutaneously and made out there for percutaneous entry to modify the fluid quantity and strain of the cuff wanted to preserve continence. For practical functions, when intermittent catheterization is required along with augmentation cystoplasty, use of native tissue for continence eliminates the long-term concern for infection or erosion and the danger of mechanical failure. Technique A Foley catheter is positioned intravesically and the bladder stuffed to capability. The bladder is exposed through either a midline or low transverse belly incision. A 6- � 2-cm rectangular flap based on the bladder neck and urethra is then isolated. Stay sutures are positioned, and the flap is mobilized in continuity with the proximal urethra. The rectangular strip primarily based on the urethra is tubularized posteriorly around the urethral catheter with a steady absorbable suture. The distal portion of the tubularized strip ought to be approximated in an interrupted style to facilitate excision of excessive tissue with out jeopardizing the suture line. A capacious submucosal tunnel by way of the trigone is then created posteriorly for the neourethra. A extensive tunnel is required to find a way to prevent kinking on the level of the bladder neck, which would impede catheterization. It is necessary to get rid of useless house on the entrance of the urethra into the bladder; this may be achieved by inserting lateral anchoring sutures in the area of the bladder neck. The detrusor tube must be pulled straight through the tunnel without curve or deviation to facilitate catheterization. When closing the bladder, the lateral wings in the region of the bladder neck are approximated and incorporate adventitia of the tubularized urethra. This enhances a watertight closure and is sustained for two to three cm anteriorly, typically as much as the area of augmentation. Because of the difficulties with catheterization, modifications of the Kropp bladder neck process have been described. They harvested an oblong strip from the anterior bladder wall much like that described by Kropp. The epithelium on the ground of the bladder is incised opposite to the tunnel made by Kropp. The tube is positioned throughout the trough with the proximal meatus secured on the ground of the bladder. The epithelial edges of the trough are then secured to the lateral aspect of the tube. As with the initial description, the suture line for tubularization of the urethra lies posteriorly in opposition to trigonal muscle. Closure of the bladder begins with reapproximation of the lateral walls of the bladder to the tube until the bladder edges meet.
Real Experiences: Customer Reviews on Zerit
Tjalf, 24 years: It is feasible that a similar cause-and-effect phenomenon happens in sacral agenesis.
Saturas, 57 years: Undescended testis is accompanied by calcitonin gene related peptide accumulation inside the sensory nucleus of the genitofemoral nerve in trans-scrotal rats.
Gorok, 51 years: However, in a nonrandomized trial of 25 kids, Sommer and colleagues (2005) discovered that therapy with oxybutynin was not related to cognitive impairment.
Deckard, 29 years: Minor criteria included decrease extremity defects in 23%, renal anomalies in 23%, ascites in 41%, widened pubic arches in 18%, narrow thorax in 9%, hydrocephalus in 9%, and a single umbilical artery in 9%.
Miguel, 34 years: Developmental adjustments in human fetal testicular cell numbers and messenger ribonucleic acid levels during the second trimester.
Nemrok, 60 years: This maneuver strikes the urethrostomy distally, lowering the size of graft needed.
10 of 10 - Review by T. Fadi
Votes: 249 votes
Total customer reviews: 249
References
- Le Treut YP, Gregoire E, Belghiti J, et al: Predictors of long-term survival after liver transplantation for metastatic endocrine tumors: An 85-case French multicentric report. Am J Transplant 8:1205, 2008.
- Bonjour JP, Bausch J, Suormala T, Baumgartner ER. Detection of biocytin in urine of children with congenital biotinidase deficiency. Intl J Vitam Nutr Res 1984;54:223.
- Nakayama M, Chen CH, Nevo E, et al: Optimal preload adjustment of maximal ventricular power index varies with cardiac chamber size, Am Heart J 136:281-288, 1998.
- Trommer BL, Homer D, Mikhael MA, Trommer BL, Homer D, Mikhael MA. Cerebral vasospasm and eclampsia. Stroke. 1988;19:326-329.
- Carcillo J Jr, Salcedo JR. Urinothorax as a manifestation of nondilated obstructive uropathy following renal transplantation. Am J Kidney Dis 1985;5(3):211-3.
- FitzGerald GA, Patrono C: The coxibs, selective inhibitors of cyclooxygenase-2, N Engl J Med 345:433, 2001.